Bryant Ng, Armeyra Devani Ferintasari, Susanna Hilda Hutajulu, Yufi Kartika Astari, Juan Adrian Wiranata, Suwardjo Suwardjo, Irianiwati Widodo, Lina Choridah, Wigati Dhamiyati, Mardiah Suci Hardianti, Kartika Widayati Taroeno-Hariadi
{"title":"Patterns, Predictors, and Prognostic Implication of Treatment-Related Amenorrhea in Patients With Breast Cancer.","authors":"Bryant Ng, Armeyra Devani Ferintasari, Susanna Hilda Hutajulu, Yufi Kartika Astari, Juan Adrian Wiranata, Suwardjo Suwardjo, Irianiwati Widodo, Lina Choridah, Wigati Dhamiyati, Mardiah Suci Hardianti, Kartika Widayati Taroeno-Hariadi","doi":"10.14740/wjon1991","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Treatment-related amenorrhea (TRA) is a common side effect of treatment in premenopausal patients with breast cancer, with important consequences for patient counseling and management. Its occurrence and potential influence on survival outcomes remain active areas of investigation. This study aimed to evaluate the incidence, risk factors, and prognostic significance of TRA in patients with breast cancer.</p><p><strong>Methods: </strong>This is a retrospective cohort study. Patients were interviewed during and after chemotherapy to assess their menstrual status. Sociodemographic, clinical, and treatment data of patients were also collected. TRA was classified into early amenorrhea (EA) and late amenorrhea (LA) based on the duration of amenorrhea. Univariable and multivariable logistic regression were used to identify risk factors of EA and LA. Kaplan-Meier curves and Cox proportional hazards analyses were used to investigate the impact of EA and LA on 3-year overall survival (OS).</p><p><strong>Results: </strong>There were 81 patients who were eligible for the final analysis. Of these subjects, 14 (17.3%) developed no amenorrhea, 67 (82.7%) developed EA, and 45 (55.6%) developed LA. We did not find any significant independent risk factor for EA. Age > 45 years (odds ratio (OR): 4.00; confidence interval (CI): 1.23 - 13.01; P = 0.021) and the usage of hormonal therapy (OR: 4.96; CI: 1.58 - 15.53; P = 0.006) independently significantly increase the risk of LA, whereas a metastatic disease status decreased the risk (OR: 0.20; CI: 0.04 - 0.90; P = 0.036). Both EA (hazard ratio (HR) = 0.262, CI: 0.105 - 0.653; P = 0.002) and LA (HR = 0.234, CI: 0.091 - 0.604; P = 0.001) were associated with an improved 3-year OS rate.</p><p><strong>Conclusions: </strong>Age > 45 years and the usage of hormonal therapy are risk factors for LA, while metastatic disease was associated with a decreased risk. Both EA and LA had a significant association with favorable 3-year OS. These findings enable clinicians to provide personalized guidance, tailor treatment strategies, and improve the outcomes of premenopausal patients with breast cancer. Standardization of how TRA is defined and assessed in future studies is essential to improve comparability and enhance the understanding of its clinical implications.</p>","PeriodicalId":46797,"journal":{"name":"World Journal of Oncology","volume":"16 2","pages":"200-209"},"PeriodicalIF":2.2000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11954610/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/wjon1991","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/18 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Treatment-related amenorrhea (TRA) is a common side effect of treatment in premenopausal patients with breast cancer, with important consequences for patient counseling and management. Its occurrence and potential influence on survival outcomes remain active areas of investigation. This study aimed to evaluate the incidence, risk factors, and prognostic significance of TRA in patients with breast cancer.
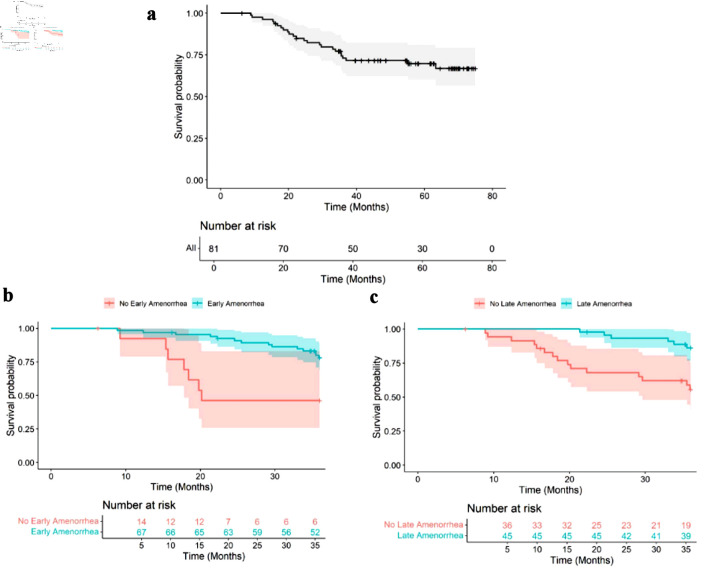
Methods: This is a retrospective cohort study. Patients were interviewed during and after chemotherapy to assess their menstrual status. Sociodemographic, clinical, and treatment data of patients were also collected. TRA was classified into early amenorrhea (EA) and late amenorrhea (LA) based on the duration of amenorrhea. Univariable and multivariable logistic regression were used to identify risk factors of EA and LA. Kaplan-Meier curves and Cox proportional hazards analyses were used to investigate the impact of EA and LA on 3-year overall survival (OS).
Results: There were 81 patients who were eligible for the final analysis. Of these subjects, 14 (17.3%) developed no amenorrhea, 67 (82.7%) developed EA, and 45 (55.6%) developed LA. We did not find any significant independent risk factor for EA. Age > 45 years (odds ratio (OR): 4.00; confidence interval (CI): 1.23 - 13.01; P = 0.021) and the usage of hormonal therapy (OR: 4.96; CI: 1.58 - 15.53; P = 0.006) independently significantly increase the risk of LA, whereas a metastatic disease status decreased the risk (OR: 0.20; CI: 0.04 - 0.90; P = 0.036). Both EA (hazard ratio (HR) = 0.262, CI: 0.105 - 0.653; P = 0.002) and LA (HR = 0.234, CI: 0.091 - 0.604; P = 0.001) were associated with an improved 3-year OS rate.
Conclusions: Age > 45 years and the usage of hormonal therapy are risk factors for LA, while metastatic disease was associated with a decreased risk. Both EA and LA had a significant association with favorable 3-year OS. These findings enable clinicians to provide personalized guidance, tailor treatment strategies, and improve the outcomes of premenopausal patients with breast cancer. Standardization of how TRA is defined and assessed in future studies is essential to improve comparability and enhance the understanding of its clinical implications.
期刊介绍:
World Journal of Oncology, bimonthly, publishes original contributions describing basic research and clinical investigation of cancer, on the cellular, molecular, prevention, diagnosis, therapy and prognosis aspects. The submissions can be basic research or clinical investigation oriented. This journal welcomes those submissions focused on the clinical trials of new treatment modalities for cancer, and those submissions focused on molecular or cellular research of the oncology pathogenesis. Case reports submitted for consideration of publication should explore either a novel genomic event/description or a new safety signal from an oncolytic agent. The areas of interested manuscripts are these disciplines: tumor immunology and immunotherapy; cancer molecular pharmacology and chemotherapy; drug sensitivity and resistance; cancer epidemiology; clinical trials; cancer pathology; radiobiology and radiation oncology; solid tumor oncology; hematological malignancies; surgical oncology; pediatric oncology; molecular oncology and cancer genes; gene therapy; cancer endocrinology; cancer metastasis; prevention and diagnosis of cancer; other cancer related subjects. The types of manuscripts accepted are original article, review, editorial, short communication, case report, letter to the editor, book review.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


