{"title":"Effects of visual guidance and instrument choice on symptom recurrence following adenoidectomy: a systematic review of randomized controlled trials.","authors":"Martin Mølhave, Therese Ovesen, Adnan Madzak","doi":"10.1136/bmjsit-2024-000370","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To assess the impact of visual guidance and instrument choice on obstructive sleep apnea (OSA) and otitis media with effusion (OME) symptom recurrence and reoperation rates following adenoidectomy in pediatric patients.</p><p><strong>Design: </strong>Systematic review of randomized controlled trials (RCTs).</p><p><strong>Setting: </strong>A comprehensive literature search was conducted in Embase, PubMed/Medline, the Cochrane Library, and Scopus, with the final search on September 23, 2024. Reference lists were also screened.</p><p><strong>Participants: </strong>Eligible studies included RCTs published from 2000 onwards, with ≥25 pediatric patients undergoing adenoidectomy for OSA or OME. Comparisons included visually guided versus blinded and cold versus hot adenoidectomy techniques. Studies involving concurrent procedures, craniofacial abnormalities, or non-primary adenoidectomy cases were excluded.</p><p><strong>Main outcome measures: </strong>The primary outcomes were OSA and OME symptom recurrence and reoperation rates following adenoidectomy. Risk of bias was assessed using Cochrane Risk of Bias tool, and evidence quality was evaluated using Grading of Recommendations Assessment, Development and Evaluation.</p><p><strong>Results: </strong>Of 2302 screened articles, 35 underwent full-text review, and 4r studies (373 participants) met inclusion criteria. All studies compared hot and cold techniques, with hot techniques being visually guided. Only one study directly compared both hot and cold techniques under visual guidance, reporting lower OSA recurrence rates with the hot technique, though with a high risk of bias. Other studies found no significant differences, and none reported reoperation rates. Study heterogeneity prevented meta-analysis. Overall risk of bias and evidence quality were moderate.</p><p><strong>Conclusions: </strong>There is insufficient evidence to determine whether visual guidance reduces symptom recurrence following adenoidectomy. Further high-quality RCTs are needed to provide more sound conclusions.</p><p><strong>Prospero registration number: </strong>CRD42024513408.</p>","PeriodicalId":33349,"journal":{"name":"BMJ Surgery Interventions Health Technologies","volume":"7 1","pages":"e000370"},"PeriodicalIF":1.6000,"publicationDate":"2025-03-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11956394/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Surgery Interventions Health Technologies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjsit-2024-000370","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To assess the impact of visual guidance and instrument choice on obstructive sleep apnea (OSA) and otitis media with effusion (OME) symptom recurrence and reoperation rates following adenoidectomy in pediatric patients.
Design: Systematic review of randomized controlled trials (RCTs).
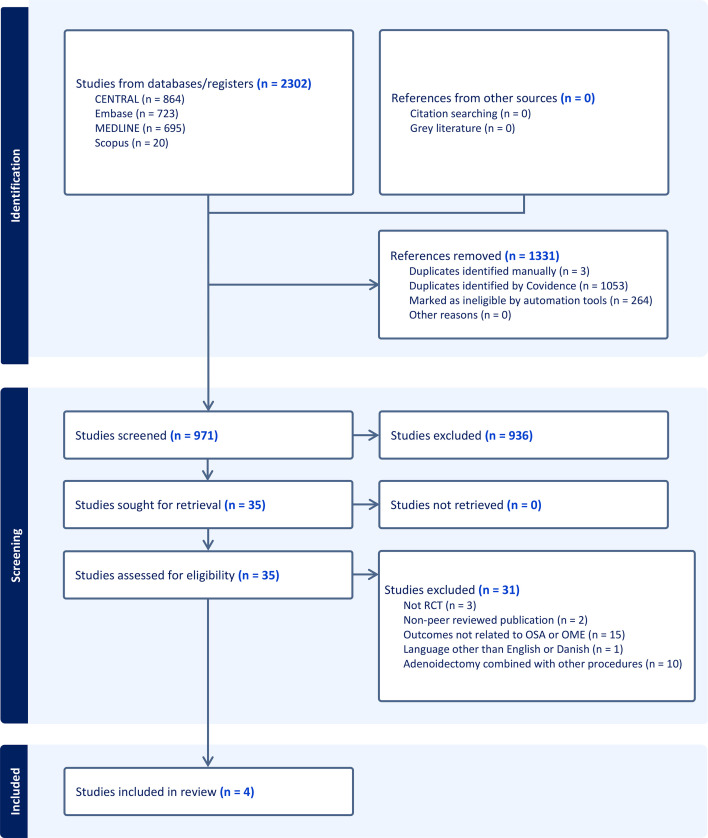
Setting: A comprehensive literature search was conducted in Embase, PubMed/Medline, the Cochrane Library, and Scopus, with the final search on September 23, 2024. Reference lists were also screened.
Participants: Eligible studies included RCTs published from 2000 onwards, with ≥25 pediatric patients undergoing adenoidectomy for OSA or OME. Comparisons included visually guided versus blinded and cold versus hot adenoidectomy techniques. Studies involving concurrent procedures, craniofacial abnormalities, or non-primary adenoidectomy cases were excluded.
Main outcome measures: The primary outcomes were OSA and OME symptom recurrence and reoperation rates following adenoidectomy. Risk of bias was assessed using Cochrane Risk of Bias tool, and evidence quality was evaluated using Grading of Recommendations Assessment, Development and Evaluation.
Results: Of 2302 screened articles, 35 underwent full-text review, and 4r studies (373 participants) met inclusion criteria. All studies compared hot and cold techniques, with hot techniques being visually guided. Only one study directly compared both hot and cold techniques under visual guidance, reporting lower OSA recurrence rates with the hot technique, though with a high risk of bias. Other studies found no significant differences, and none reported reoperation rates. Study heterogeneity prevented meta-analysis. Overall risk of bias and evidence quality were moderate.
Conclusions: There is insufficient evidence to determine whether visual guidance reduces symptom recurrence following adenoidectomy. Further high-quality RCTs are needed to provide more sound conclusions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


