Candice L Wilshire, Kerrie E Buehler, Claire A Henson, Christopher R Gilbert, Jed A Gorden
{"title":"Community-Based Lung Cancer Screening Program Structure, Quality, and Barriers: The Struggle for Implementation.","authors":"Candice L Wilshire, Kerrie E Buehler, Claire A Henson, Christopher R Gilbert, Jed A Gorden","doi":"10.1155/carj/9683951","DOIUrl":null,"url":null,"abstract":"<p><p><b>Objectives:</b> Recommendations for programmatic components for lung cancer screening programs (LCSPs) have been published; however, adoption within LCSPs has not been mandated and implementation requires resources. We aimed to determine the presence of recommended structural and quality elements within LCSPs and determine barriers to performing LCS within a community-based, multistate healthcare network. <b>Methods:</b> We conducted a cross-sectional study using two structured interviews within a community-based healthcare network between 1 June 2018 and 31 July 2020. Two separate interviews were created, one delivered to LCSP navigators to determine the presence of recommended structural and quality elements within LCSPs and one delivered to imaging center administrators to determine barriers to LCS implementation. <b>Results:</b> Of the 22 LCSPs, 20 (91%) were decentralized and 2 (9%) centralized. Three (14%) utilized standardized shared decision-making tools and 13 (59%) a multidisciplinary nodule review. Of the 21 (95%) LCSPs who collected information for external purposes, 9 (43%) collected it manually. Ten (45%) utilized a standard procedure for smoking cessation, and 5 (23%) had Certified Tobacco Treatment Specialists. Of the 31 affiliated imaging sites not associated with a LCSP, 8 (26%) were performing LCS. While 19 (61%) sites had the resources to fulfill or maintain an increase in LCS orders, lack of resources was the predominant (11, 35%) barrier to implementing a LCSP. <b>Conclusions:</b> A wide variation in the structure, quality, and resource allocation was identified within the network of LCSPs. Further research identifying the implications this variation has on outcomes, operational cost, and experience may shed light on whether stringent program quality control is needed.</p>","PeriodicalId":9416,"journal":{"name":"Canadian respiratory journal","volume":"2025 ","pages":"9683951"},"PeriodicalIF":2.1000,"publicationDate":"2025-03-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11952916/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian respiratory journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/carj/9683951","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
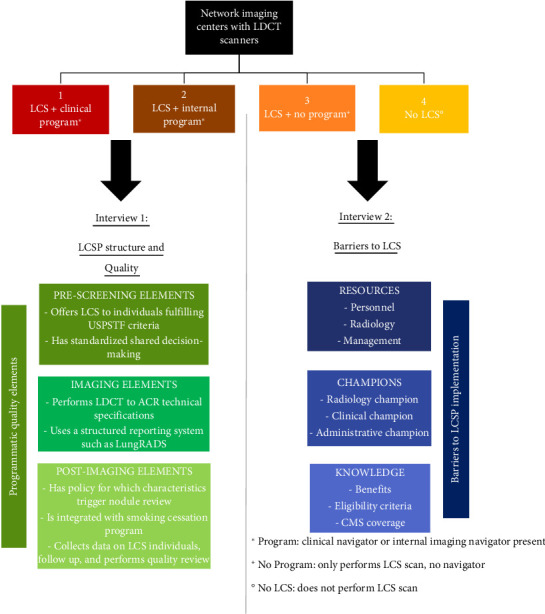
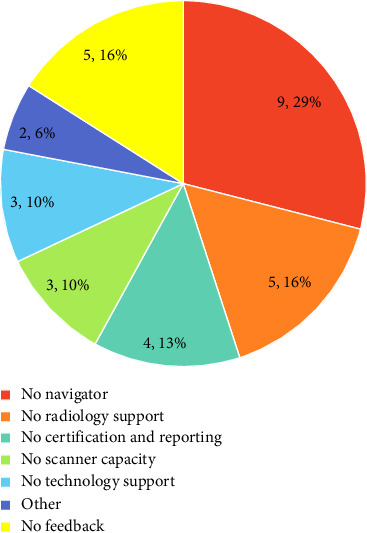
Objectives: Recommendations for programmatic components for lung cancer screening programs (LCSPs) have been published; however, adoption within LCSPs has not been mandated and implementation requires resources. We aimed to determine the presence of recommended structural and quality elements within LCSPs and determine barriers to performing LCS within a community-based, multistate healthcare network. Methods: We conducted a cross-sectional study using two structured interviews within a community-based healthcare network between 1 June 2018 and 31 July 2020. Two separate interviews were created, one delivered to LCSP navigators to determine the presence of recommended structural and quality elements within LCSPs and one delivered to imaging center administrators to determine barriers to LCS implementation. Results: Of the 22 LCSPs, 20 (91%) were decentralized and 2 (9%) centralized. Three (14%) utilized standardized shared decision-making tools and 13 (59%) a multidisciplinary nodule review. Of the 21 (95%) LCSPs who collected information for external purposes, 9 (43%) collected it manually. Ten (45%) utilized a standard procedure for smoking cessation, and 5 (23%) had Certified Tobacco Treatment Specialists. Of the 31 affiliated imaging sites not associated with a LCSP, 8 (26%) were performing LCS. While 19 (61%) sites had the resources to fulfill or maintain an increase in LCS orders, lack of resources was the predominant (11, 35%) barrier to implementing a LCSP. Conclusions: A wide variation in the structure, quality, and resource allocation was identified within the network of LCSPs. Further research identifying the implications this variation has on outcomes, operational cost, and experience may shed light on whether stringent program quality control is needed.
期刊介绍:
Canadian Respiratory Journal is a peer-reviewed, Open Access journal that aims to provide a multidisciplinary forum for research in all areas of respiratory medicine. The journal publishes original research articles, review articles, and clinical studies related to asthma, allergy, COPD, non-invasive ventilation, therapeutic intervention, lung cancer, airway and lung infections, as well as any other respiratory diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


