Associations between clozapine availability, the diagnosis of treatment-resistant schizophrenia subgroups, antipsychotic monotherapy, and concomitant psychotropics among patients with schizophrenia: a real-world nationwide study.
{"title":"Associations between clozapine availability, the diagnosis of treatment-resistant schizophrenia subgroups, antipsychotic monotherapy, and concomitant psychotropics among patients with schizophrenia: a real-world nationwide study.","authors":"Shinichiro Ochi, Fumitoshi Kodaka, Naomi Hasegawa, Takashi Tsuboi, Kazutaka Ohi, Shun Igarashi, Kentaro Fukumoto, Jun-Ichi Iga, Hiroyuki Muraoka, Hitoshi Iida, Hiromi Tagata, Hiroko Kashiwagi, Shusuke Numata, Hirotaka Yamagata, Masahiro Takeshima, Kayo Ichihashi, Naoki Hashimoto, Tatsuya Nagasawa, Toshinori Nakamura, Junya Matsumoto, Hisashi Yamada, Hikaru Hori, Shu-Ichi Ueno, Ken Inada, Ryota Hashimoto, Norio Yasui-Furukori","doi":"10.1093/ijnp/pyaf011","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and hypothesis: </strong>The rate of antipsychotic polypharmacy is high. One risk factor for antipsychotic polypharmacy may be the severity of schizophrenia, including treatment-resistant schizophrenia (TRS). We hypothesized that the institutions that are able to prescribe clozapine present differences in pharmacological treatment even before TRS is diagnosed.</p><p><strong>Study design: </strong>A total of 8155 patients with schizophrenia were divided into the clozapine-available institution (CAI) group and the clozapine-unavailable institution (CUI) group. The psychotropic prescription rates at discharge were compared between the two groups. Furthermore, to investigate whether the diagnosis of TRS subgroups influenced treatment efficacy, we compared CAIs and CUIs with descriptions of subgroups with TRS (DSTRS) and those without descriptions of subgroups with TRS (NDSTRS).</p><p><strong>Results: </strong>Compared to the CUI group, the rates of both antipsychotic monotherapy (58.3% vs. 50.7%; P = 2.4 × 10-7) and antipsychotic monotherapy without the concomitant use of other psychotropics (20.4% vs. 15.6%; P = 3.8 × 10-5) were significantly higher in the CAI group. The rate of antipsychotic monotherapy in the CAI with DSTRS group (63.3%) was significantly higher than that in the CAI with NDSTRS group (54.5%; P = 1.4 × 10-12), the CUI with DSTRS group (49.6%; P = 4.9 × 10-9), and the CUI with NDSTRS group (50.9%; P = 2.0 × 10-8). The rate of antipsychotic monotherapy without the concomitant use of other psychotropics in the CAI with DSTRS group (22.6%) was also significantly higher than that in the CAI with NDSTRS group (18.7%; P = 4.7 × 10-4), the CUI with DSTRS group (15.9%; P = 5.5 × 10-4), and the CUI with NDSTRS group (15.2%; P = 8.0 × 10-5). There was no significant difference in these rates between the other groups.</p><p><strong>Conclusions: </strong>Both the availability of clozapine prescriptions and the precise diagnosis of TRS subgroups at discharge can promote the development of an organizational culture that facilitates the treatment of patients with schizophrenia.</p>","PeriodicalId":14134,"journal":{"name":"International Journal of Neuropsychopharmacology","volume":" ","pages":""},"PeriodicalIF":3.7000,"publicationDate":"2025-04-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11986582/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Neuropsychopharmacology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ijnp/pyaf011","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and hypothesis: The rate of antipsychotic polypharmacy is high. One risk factor for antipsychotic polypharmacy may be the severity of schizophrenia, including treatment-resistant schizophrenia (TRS). We hypothesized that the institutions that are able to prescribe clozapine present differences in pharmacological treatment even before TRS is diagnosed.
Study design: A total of 8155 patients with schizophrenia were divided into the clozapine-available institution (CAI) group and the clozapine-unavailable institution (CUI) group. The psychotropic prescription rates at discharge were compared between the two groups. Furthermore, to investigate whether the diagnosis of TRS subgroups influenced treatment efficacy, we compared CAIs and CUIs with descriptions of subgroups with TRS (DSTRS) and those without descriptions of subgroups with TRS (NDSTRS).
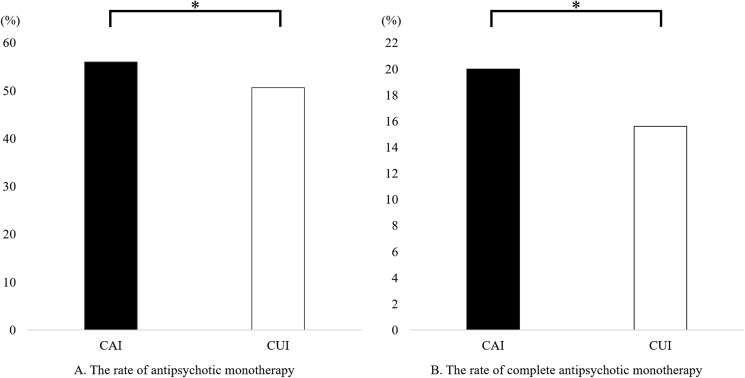
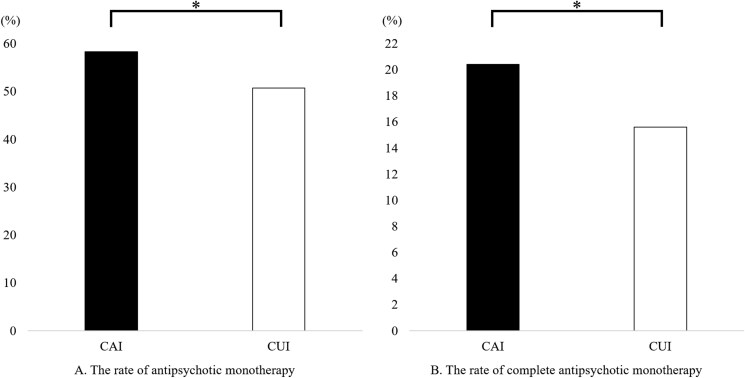
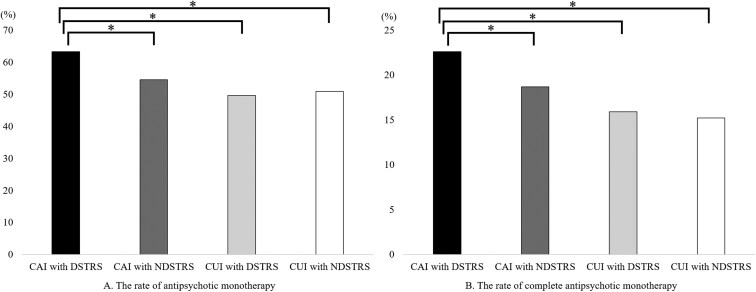
Results: Compared to the CUI group, the rates of both antipsychotic monotherapy (58.3% vs. 50.7%; P = 2.4 × 10-7) and antipsychotic monotherapy without the concomitant use of other psychotropics (20.4% vs. 15.6%; P = 3.8 × 10-5) were significantly higher in the CAI group. The rate of antipsychotic monotherapy in the CAI with DSTRS group (63.3%) was significantly higher than that in the CAI with NDSTRS group (54.5%; P = 1.4 × 10-12), the CUI with DSTRS group (49.6%; P = 4.9 × 10-9), and the CUI with NDSTRS group (50.9%; P = 2.0 × 10-8). The rate of antipsychotic monotherapy without the concomitant use of other psychotropics in the CAI with DSTRS group (22.6%) was also significantly higher than that in the CAI with NDSTRS group (18.7%; P = 4.7 × 10-4), the CUI with DSTRS group (15.9%; P = 5.5 × 10-4), and the CUI with NDSTRS group (15.2%; P = 8.0 × 10-5). There was no significant difference in these rates between the other groups.
Conclusions: Both the availability of clozapine prescriptions and the precise diagnosis of TRS subgroups at discharge can promote the development of an organizational culture that facilitates the treatment of patients with schizophrenia.
期刊介绍:
The central focus of the journal is on research that advances understanding of existing and new neuropsychopharmacological agents including their mode of action and clinical application or provides insights into the biological basis of psychiatric disorders and thereby advances their pharmacological treatment. Such research may derive from the full spectrum of biological and psychological fields of inquiry encompassing classical and novel techniques in neuropsychopharmacology as well as strategies such as neuroimaging, genetics, psychoneuroendocrinology and neuropsychology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


