Ahmad Kaleem, Deema Othman, Carlos Yanez, Jody Miller
{"title":"Acute Internal Pelvic Hernia: A Complex Diagnostic Challenge.","authors":"Ahmad Kaleem, Deema Othman, Carlos Yanez, Jody Miller","doi":"10.4293/CRSLS.2024.00074","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Internal abdominopelvic hernias, whether congenital or acquired, are a rare cause of acute small bowel obstruction. Symptoms range from recurrent abdominal pain to acute obstruction, which can lead to severe complications like bowel ischemia, perforation, or death if untreated. Diagnosis is often difficult due to variable symptoms, but prompt surgical intervention is crucial to prevent life-threatening outcomes.</p><p><strong>Case description: </strong>We treated a 42-year-old female airline cabin crew member who presented with colicky abdominal pain, bilious vomiting, and lower abdominal tenderness. Her abdominal computed tomography (CT) scan showed small bowel obstruction with loops of small bowel predominantly in the left lower abdomen. She had a history of a single episode of similar abdominal pain many years prior, which resolved spontaneously. The rest of her history was unremarkable. She received nonoperative management initially, but due to persistent abdominal pain and vomiting, a diagnostic laparoscopy was done. The diagnostic laparoscopy showed congested but viable small bowel herniating into a peritoneal defect through the lateral part of left broad ligament at the lateral pelvic wall into the retroperitoneum. The hernia was reduced, and the defect was repaired. Postoperatively, she had an uncomplicated recovery.</p><p><strong>Discussion: </strong>Internal hernia is an important differential diagnosis in patients presenting with an acute abdomen, especially with a history of recurrent small bowel obstructions, regardless of surgical history. Physicians need to have a high index of suspicion to diagnose and treat this condition without delay, preventing morbidity and mortality in this patient group.</p>","PeriodicalId":72723,"journal":{"name":"CRSLS : MIS case reports from SLS","volume":"12 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-03-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11938174/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CRSLS : MIS case reports from SLS","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4293/CRSLS.2024.00074","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Internal abdominopelvic hernias, whether congenital or acquired, are a rare cause of acute small bowel obstruction. Symptoms range from recurrent abdominal pain to acute obstruction, which can lead to severe complications like bowel ischemia, perforation, or death if untreated. Diagnosis is often difficult due to variable symptoms, but prompt surgical intervention is crucial to prevent life-threatening outcomes.
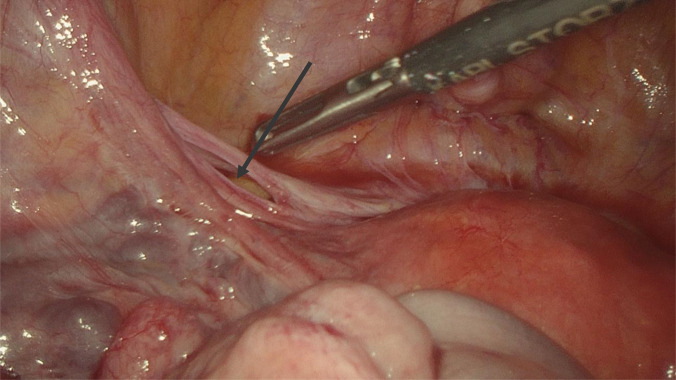
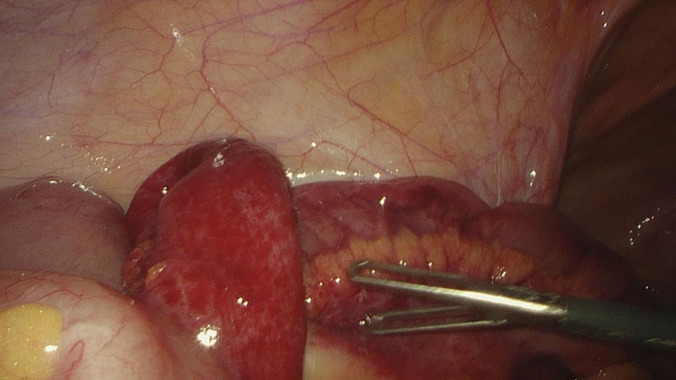
Case description: We treated a 42-year-old female airline cabin crew member who presented with colicky abdominal pain, bilious vomiting, and lower abdominal tenderness. Her abdominal computed tomography (CT) scan showed small bowel obstruction with loops of small bowel predominantly in the left lower abdomen. She had a history of a single episode of similar abdominal pain many years prior, which resolved spontaneously. The rest of her history was unremarkable. She received nonoperative management initially, but due to persistent abdominal pain and vomiting, a diagnostic laparoscopy was done. The diagnostic laparoscopy showed congested but viable small bowel herniating into a peritoneal defect through the lateral part of left broad ligament at the lateral pelvic wall into the retroperitoneum. The hernia was reduced, and the defect was repaired. Postoperatively, she had an uncomplicated recovery.
Discussion: Internal hernia is an important differential diagnosis in patients presenting with an acute abdomen, especially with a history of recurrent small bowel obstructions, regardless of surgical history. Physicians need to have a high index of suspicion to diagnose and treat this condition without delay, preventing morbidity and mortality in this patient group.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


