Gwenllian Wilkinson, Ayodele Sasegbon, Craig J Smith, Philip M Bath, Shaheen Hamdy
{"title":"Feasibility of Cerebellar Stimulation for the Treatment of Post-Stroke Dysphagia.","authors":"Gwenllian Wilkinson, Ayodele Sasegbon, Craig J Smith, Philip M Bath, Shaheen Hamdy","doi":"10.1007/s12311-025-01823-0","DOIUrl":null,"url":null,"abstract":"<p><p>Post-stroke dysphagia (PSD) is common and associated with poor outcomes. We aimed to explore the feasibility, safety, and proof of concept of cerebellar rTMS in patients with sub-acute PSD. We intended to recruit 48 participants with PSD. Randomised to: (i) sham treatment twice-daily for five days, (ii) cerebellar rTMS daily for three days, and (iii) cerebellar rTMS twice-daily for five days (1:1:1). Participants were blinded to treatment group. Primary outcomes were feasibility, safety, and functional outcome intake scale (FOIS), dysphagia severity rating scale (DSRS), and feeding status scale (FSS) at two weeks. However, due to lower-than-expected enrolment, the active rTMS groups were combined. We recruited 14 participants in total, (mean 68 years, 57% female). Due to the time-limited funding period, recruitment was adversely affected by the COVID-19 pandemic. DSRS and FSS trended lower in the combined active rTMS groups at two weeks, i.e. less swallowing impairment. However, at death/discharge FOIS was higher/better (mean, (standard deviation)), 4.0 (2.1) vs. 1.8 (1.0) (p = 0.032) with active TMS, with trends to lower/better DSRS and FSS. There was no difference in the acceptability of treatment between groups. High-intensity (n = 5) vs. low-intensity (n = 5) cerebellar rTMS was associated with lower DSRS 3.0 (1.4) vs. 9.4 (2.7) and FSS 0.6 (0.5) vs. 1.6 (0.5) at 2 weeks, and DSRS 3.0 (1.4) vs. 9.0 (3.7) at hospital discharge or death. Cerebellar rTMS is a feasible ward-based treatment for reducing swallowing impairment. Although enrolment was lower than desired, there was evidence for proof of concept, particularly for high-intensity cerebellar rTMS. Larger studies are warranted.</p>","PeriodicalId":50706,"journal":{"name":"Cerebellum","volume":"24 3","pages":"74"},"PeriodicalIF":2.4000,"publicationDate":"2025-03-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11946963/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cerebellum","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12311-025-01823-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"NEUROSCIENCES","Score":null,"Total":0}
引用次数: 0
Abstract
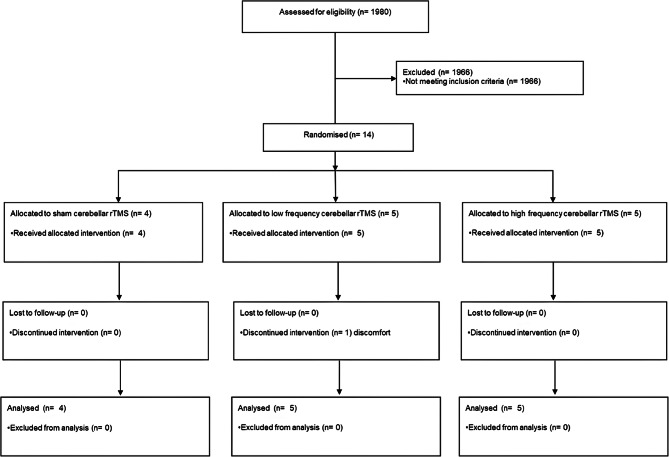
Post-stroke dysphagia (PSD) is common and associated with poor outcomes. We aimed to explore the feasibility, safety, and proof of concept of cerebellar rTMS in patients with sub-acute PSD. We intended to recruit 48 participants with PSD. Randomised to: (i) sham treatment twice-daily for five days, (ii) cerebellar rTMS daily for three days, and (iii) cerebellar rTMS twice-daily for five days (1:1:1). Participants were blinded to treatment group. Primary outcomes were feasibility, safety, and functional outcome intake scale (FOIS), dysphagia severity rating scale (DSRS), and feeding status scale (FSS) at two weeks. However, due to lower-than-expected enrolment, the active rTMS groups were combined. We recruited 14 participants in total, (mean 68 years, 57% female). Due to the time-limited funding period, recruitment was adversely affected by the COVID-19 pandemic. DSRS and FSS trended lower in the combined active rTMS groups at two weeks, i.e. less swallowing impairment. However, at death/discharge FOIS was higher/better (mean, (standard deviation)), 4.0 (2.1) vs. 1.8 (1.0) (p = 0.032) with active TMS, with trends to lower/better DSRS and FSS. There was no difference in the acceptability of treatment between groups. High-intensity (n = 5) vs. low-intensity (n = 5) cerebellar rTMS was associated with lower DSRS 3.0 (1.4) vs. 9.4 (2.7) and FSS 0.6 (0.5) vs. 1.6 (0.5) at 2 weeks, and DSRS 3.0 (1.4) vs. 9.0 (3.7) at hospital discharge or death. Cerebellar rTMS is a feasible ward-based treatment for reducing swallowing impairment. Although enrolment was lower than desired, there was evidence for proof of concept, particularly for high-intensity cerebellar rTMS. Larger studies are warranted.
期刊介绍:
Official publication of the Society for Research on the Cerebellum devoted to genetics of cerebellar ataxias, role of cerebellum in motor control and cognitive function, and amid an ageing population, diseases associated with cerebellar dysfunction.
The Cerebellum is a central source for the latest developments in fundamental neurosciences including molecular and cellular biology; behavioural neurosciences and neurochemistry; genetics; fundamental and clinical neurophysiology; neurology and neuropathology; cognition and neuroimaging.
The Cerebellum benefits neuroscientists in molecular and cellular biology; neurophysiologists; researchers in neurotransmission; neurologists; radiologists; paediatricians; neuropsychologists; students of neurology and psychiatry and others.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


