Oskari Pakarinen, Matti Ahonen, Petra Grahn, Ilkka Helenius, Topi Laaksonen
{"title":"Refractures in Children.","authors":"Oskari Pakarinen, Matti Ahonen, Petra Grahn, Ilkka Helenius, Topi Laaksonen","doi":"10.2106/JBJS.24.01014","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Fractures are common in children, but knowledge about refractures has been limited. This study aimed to determine the rate of radiographically confirmed refractures within 2 years of the primary fracture in children and to analyze the association between fracture stability and refracture risk.</p><p><strong>Methods: </strong>All patients who were <16 years of age and had at least 2 fractures in the same bone between 2014 and 2023 were reviewed from the Helsinki University Hospitals' electronic pediatric treatment register, KIDS Fracture Tool. Patients' radiographs and records were evaluated. Patients with subsequent fractures in different parts of the bone than the primary fracture, patients with pathological fractures, and patients with a systemic condition predisposing to fractures were excluded.</p><p><strong>Results: </strong>Of 20,749 fractures, 163 consecutive fractures in the same bone within 2 years were identified. After exclusions, 100 cases (0.48% of all fractures) remained, with 83 occurring within 1 year and 17 occurring in the second year after the primary fracture. Refracture rates were highest in diaphyseal both-bone forearm fractures (3.76% [43 of 1,144]), diaphyseal tibial fractures (1.01% [7 of 693]), distal forearm fractures (0.55% [27 of 4,949]), and distal humeral fractures (0.49% [11 of 2,227]). The median time to refracture was 73 days (interquartile range [IQR], 56 to 131 days) for the distal forearm, 109 days (IQR, 79 to 169 days) for the diaphyseal tibia, 124 days (IQR, 80 to 178 days) for the diaphyseal forearm, and 426 days (IQR, 243 to 660 days) for the distal humerus. Displaced fractures requiring closed reduction had a significantly higher refracture risk compared with other fractures: relative risk (RR), 8.0 (95% confidence interval [CI], 4.5 to 14) compared with stable fractures; RR, 5.0 (95% CI, 2.9 to 8.7) compared with fractures that had acceptable position but might be unstable and required follow-up; and RR, 3.2 (95% CI, 1.8 to 5.7) compared with fractures requiring fixation and follow-up.</p><p><strong>Conclusions: </strong>The overall refracture rate in children was approximately 0.5%, with the highest rates in both-bone diaphyseal forearm fractures. The median time to refracture varied significantly by anatomic location, and displaced fractures treated with closed reduction were associated with a higher refracture risk.</p><p><strong>Level of evidence: </strong>Therapeutic Level III . See Instructions for Authors for a complete description of levels of evidence.</p>","PeriodicalId":15273,"journal":{"name":"Journal of Bone and Joint Surgery, American Volume","volume":" ","pages":"e40"},"PeriodicalIF":4.3000,"publicationDate":"2025-05-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12047644/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Bone and Joint Surgery, American Volume","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2106/JBJS.24.01014","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/27 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Fractures are common in children, but knowledge about refractures has been limited. This study aimed to determine the rate of radiographically confirmed refractures within 2 years of the primary fracture in children and to analyze the association between fracture stability and refracture risk.
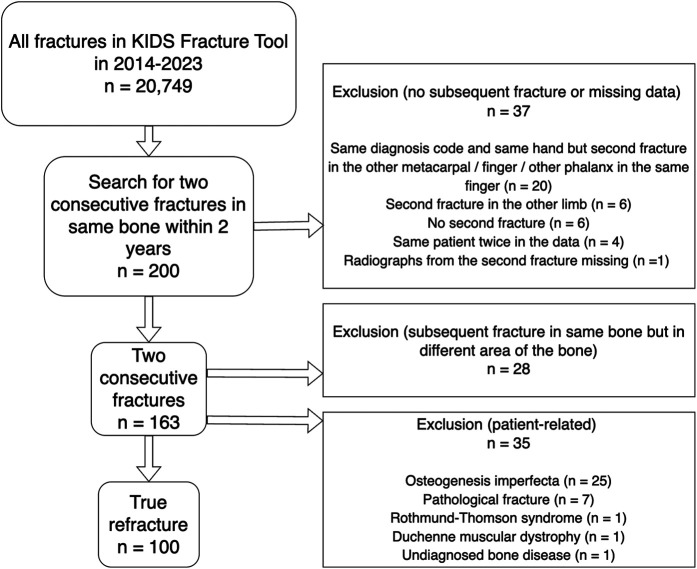
Methods: All patients who were <16 years of age and had at least 2 fractures in the same bone between 2014 and 2023 were reviewed from the Helsinki University Hospitals' electronic pediatric treatment register, KIDS Fracture Tool. Patients' radiographs and records were evaluated. Patients with subsequent fractures in different parts of the bone than the primary fracture, patients with pathological fractures, and patients with a systemic condition predisposing to fractures were excluded.
Results: Of 20,749 fractures, 163 consecutive fractures in the same bone within 2 years were identified. After exclusions, 100 cases (0.48% of all fractures) remained, with 83 occurring within 1 year and 17 occurring in the second year after the primary fracture. Refracture rates were highest in diaphyseal both-bone forearm fractures (3.76% [43 of 1,144]), diaphyseal tibial fractures (1.01% [7 of 693]), distal forearm fractures (0.55% [27 of 4,949]), and distal humeral fractures (0.49% [11 of 2,227]). The median time to refracture was 73 days (interquartile range [IQR], 56 to 131 days) for the distal forearm, 109 days (IQR, 79 to 169 days) for the diaphyseal tibia, 124 days (IQR, 80 to 178 days) for the diaphyseal forearm, and 426 days (IQR, 243 to 660 days) for the distal humerus. Displaced fractures requiring closed reduction had a significantly higher refracture risk compared with other fractures: relative risk (RR), 8.0 (95% confidence interval [CI], 4.5 to 14) compared with stable fractures; RR, 5.0 (95% CI, 2.9 to 8.7) compared with fractures that had acceptable position but might be unstable and required follow-up; and RR, 3.2 (95% CI, 1.8 to 5.7) compared with fractures requiring fixation and follow-up.
Conclusions: The overall refracture rate in children was approximately 0.5%, with the highest rates in both-bone diaphyseal forearm fractures. The median time to refracture varied significantly by anatomic location, and displaced fractures treated with closed reduction were associated with a higher refracture risk.
Level of evidence: Therapeutic Level III . See Instructions for Authors for a complete description of levels of evidence.
期刊介绍:
The Journal of Bone & Joint Surgery (JBJS) has been the most valued source of information for orthopaedic surgeons and researchers for over 125 years and is the gold standard in peer-reviewed scientific information in the field. A core journal and essential reading for general as well as specialist orthopaedic surgeons worldwide, The Journal publishes evidence-based research to enhance the quality of care for orthopaedic patients. Standards of excellence and high quality are maintained in everything we do, from the science of the content published to the customer service we provide. JBJS is an independent, non-profit journal.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


