Karl Teurneau-Hermansson, David von Rosen, Jacob Ede, Mårten Larsson, Johan Sjögren, Per Wierup, Shahab Nozohoor, Igor Zindovic
{"title":"Causes and clinical impact of initial misdiagnosis of acute type A aortic dissection.","authors":"Karl Teurneau-Hermansson, David von Rosen, Jacob Ede, Mårten Larsson, Johan Sjögren, Per Wierup, Shahab Nozohoor, Igor Zindovic","doi":"10.1093/ehjopen/oeaf027","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>The high mortality in untreated acute type A aortic dissection (ATAAD) stresses the need for prompt diagnosis and immediate surgical treatment. Our aim was to evaluate the frequency and clinical impact of misdiagnosis and delayed diagnosis of ATAAD.</p><p><strong>Methods and results: </strong>This was a single-centre, retrospective, observational study including all ATAAD patients with available admission charts between 2001 and 2021 in an area of 1.9 million inhabitants in southern Sweden. The primary endpoints were initial misdiagnosis, delayed diagnosis, and 30-day mortality. Surgical treatment was a secondary endpoint. Independent predictors of misdiagnosis and 30-day mortality were identified by multivariable logistic regression and subgroup analyses by severity of clinical presentation were performed. There were 556 patients included in the study (418 surgically treated and 138 non-surgically treated), and 45.3% were initially misdiagnosed. Misdiagnosed patients were more often female (47.6 vs. 35.9%; <i>P</i> = 0.005) and demonstrated significantly lower rates of syncope, hypotensive shock, and malperfusion. Patients without signs of malperfusion subjected to diagnostic delay were less likely offered surgical treatment (74.0 vs. 91.5%; <i>P</i> < 0.001) and had higher 30-day mortality (21.3 vs. 10.8%; <i>P</i> = 0.040). Female sex was an independent predictor of misdiagnosis (OR: 1.748; 95% CI 1.145-2.668; <i>P</i> = 0.010), but neither misdiagnosis nor delayed diagnosis were independent predictors of 30-day mortality.</p><p><strong>Conclusion: </strong>Although misdiagnosis and delayed diagnosis did not influence overall 30-day mortality, delayed diagnosis led to significantly higher 30-day mortality in the large group of patients presenting without signs of malperfusion, likely caused by the observed higher risk of being denied surgical treatment.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 2","pages":"oeaf027"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11935741/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf027","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: The high mortality in untreated acute type A aortic dissection (ATAAD) stresses the need for prompt diagnosis and immediate surgical treatment. Our aim was to evaluate the frequency and clinical impact of misdiagnosis and delayed diagnosis of ATAAD.
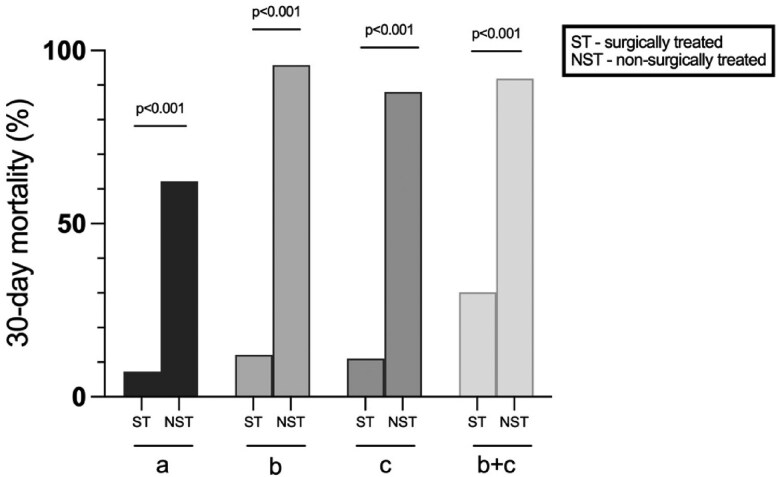
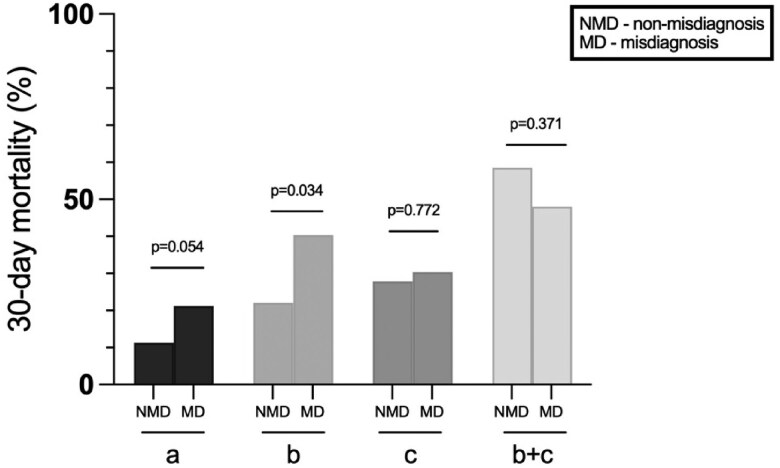
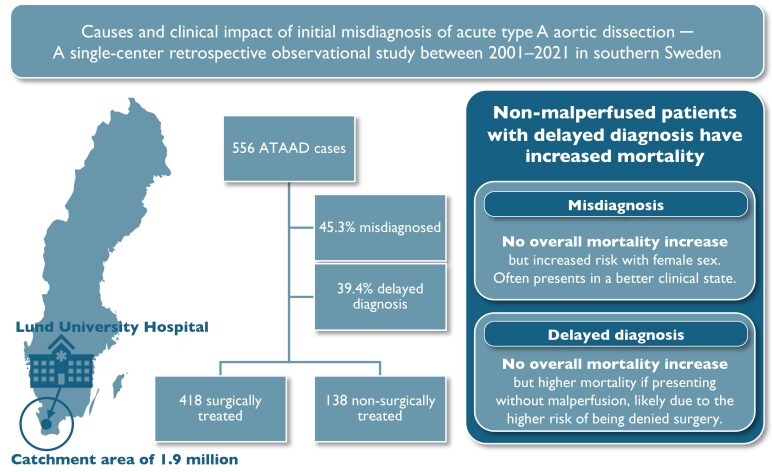
Methods and results: This was a single-centre, retrospective, observational study including all ATAAD patients with available admission charts between 2001 and 2021 in an area of 1.9 million inhabitants in southern Sweden. The primary endpoints were initial misdiagnosis, delayed diagnosis, and 30-day mortality. Surgical treatment was a secondary endpoint. Independent predictors of misdiagnosis and 30-day mortality were identified by multivariable logistic regression and subgroup analyses by severity of clinical presentation were performed. There were 556 patients included in the study (418 surgically treated and 138 non-surgically treated), and 45.3% were initially misdiagnosed. Misdiagnosed patients were more often female (47.6 vs. 35.9%; P = 0.005) and demonstrated significantly lower rates of syncope, hypotensive shock, and malperfusion. Patients without signs of malperfusion subjected to diagnostic delay were less likely offered surgical treatment (74.0 vs. 91.5%; P < 0.001) and had higher 30-day mortality (21.3 vs. 10.8%; P = 0.040). Female sex was an independent predictor of misdiagnosis (OR: 1.748; 95% CI 1.145-2.668; P = 0.010), but neither misdiagnosis nor delayed diagnosis were independent predictors of 30-day mortality.
Conclusion: Although misdiagnosis and delayed diagnosis did not influence overall 30-day mortality, delayed diagnosis led to significantly higher 30-day mortality in the large group of patients presenting without signs of malperfusion, likely caused by the observed higher risk of being denied surgical treatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


