International Validation and Refinement of Oncological Borderline Resectability Criteria for Hepatocellular Carcinoma Using Tumor Burden Score to Predict Survival.
Miho Akabane, Jun Kawashima, Abdullah Altaf, Selamawit Woldesenbet, François Cauchy, Federico Aucejo, Irinel Popescu, Minoru Kitago, Guillaume Martel, Francesca Ratti, Luca Aldrighetti, George A Poultsides, Yuki Imaoka, Andrea Ruzzenente, Itaru Endo, Ana Gleisner, Hugo P Marques, Sara Oliveira, Jorge Balaia, Vincent Lam, Tom Hugh, Nazim Bhimani, Feng Shen, Timothy M Pawlik
{"title":"International Validation and Refinement of Oncological Borderline Resectability Criteria for Hepatocellular Carcinoma Using Tumor Burden Score to Predict Survival.","authors":"Miho Akabane, Jun Kawashima, Abdullah Altaf, Selamawit Woldesenbet, François Cauchy, Federico Aucejo, Irinel Popescu, Minoru Kitago, Guillaume Martel, Francesca Ratti, Luca Aldrighetti, George A Poultsides, Yuki Imaoka, Andrea Ruzzenente, Itaru Endo, Ana Gleisner, Hugo P Marques, Sara Oliveira, Jorge Balaia, Vincent Lam, Tom Hugh, Nazim Bhimani, Feng Shen, Timothy M Pawlik","doi":"10.1097/AS9.0000000000000557","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The aim of this study is to externally validate the original borderline resectability (BR) category for predicting overall survival (OS) in hepatocellular carcinoma (HCC) following resection and to assess whether incorporating the tumor burden score (TBS) and other clinical factors could enhance predictive accuracy.</p><p><strong>Background: </strong>A recent Japanese expert panel introduced a new HCC classification scheme: resectable (R), borderline resectable 1 (BR1), and borderline resectable 2 (BR2).</p><p><strong>Methods: </strong>Patients undergoing curative-intent hepatectomy for HCC (2000-2023) were classified as R, BR1, and BR2 using the original BR and a novel TBS-BR category. The TBS-BR category replaces BR's categorical tumor morphology factors with the continuous TBS (TBS² = [maximum tumor diameter]² + [number of tumors]²). Multivariable analysis identified oncologic, morphometric, and patient-level factors associated with OS, which were incorporated into an online predictive tool.</p><p><strong>Results: </strong>Among 1766 patients, the original BR category grouped 1504 (85.2%) as R, 249 (14.1%) as BR1, and 13 (0.7%) as BR2. Utilizing the TBS-BR category, patients were reclassified as TBS-BR R (n = 684, 38.7%), BR1 (n = 1009, 57.1%), and BR2 (n = 73, 4.1%). Both the original and TBS-BR categories correlated with 5-year OS (original: 65.1%, 48.2%, 46.4%; TBS-BR: 70.8%, 58.3%, 40.0%; <i>P</i> < 0.001 for both; area under the curve: 0.54 vs 0.58). On multivariable analysis, TBS-BR1 (hazard ratio [HR]: 1.59 [1.20-2.09]; <i>P</i> = 0.001), TBS-BR2 (HR: 2.45 [1.47-4.07]; <i>P</i> < 0.001, reference: TBS-BR R), American Society of Anesthesiologists (ASA) class >2 (HR: 1.40 [1.09-1.80]; <i>P</i> = 0.007), albumin-bilirubin (ALBI) score (HR: 1.51 [1.21-1.88]; <i>P</i> < 0.001), and log <i>α</i>-fetoprotein (AFP) (HR: 1.07 [1.03-1.11]; <i>P</i> < 0.001) were independently associated with OS. A TBS-BR composite model based on these factors (TBS-BR category, ASA class, ALBI score, and log AFP) was developed and made available online (https://makbn.shinyapps.io/BRHCC/). The model's area under the receiver operating characteristic at 5 years (0.70) outperformed both the original BR (0.57) and Barcelona Clinic Liver Cancer classification (0.64).</p><p><strong>Conclusions: </strong>The TBS-BR composite model, integrating tumor morphology (TBS), tumor biology (log AFP), overall physical status (ASA class), and liver function (ALBI score) demonstrated superior predictive accuracy for OS compared with the original BR and Barcelona Clinic Liver Cancer classifications.</p>","PeriodicalId":72231,"journal":{"name":"Annals of surgery open : perspectives of surgical history, education, and clinical approaches","volume":"6 1","pages":"e557"},"PeriodicalIF":0.0000,"publicationDate":"2025-02-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11932596/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of surgery open : perspectives of surgical history, education, and clinical approaches","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/AS9.0000000000000557","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: The aim of this study is to externally validate the original borderline resectability (BR) category for predicting overall survival (OS) in hepatocellular carcinoma (HCC) following resection and to assess whether incorporating the tumor burden score (TBS) and other clinical factors could enhance predictive accuracy.
Background: A recent Japanese expert panel introduced a new HCC classification scheme: resectable (R), borderline resectable 1 (BR1), and borderline resectable 2 (BR2).
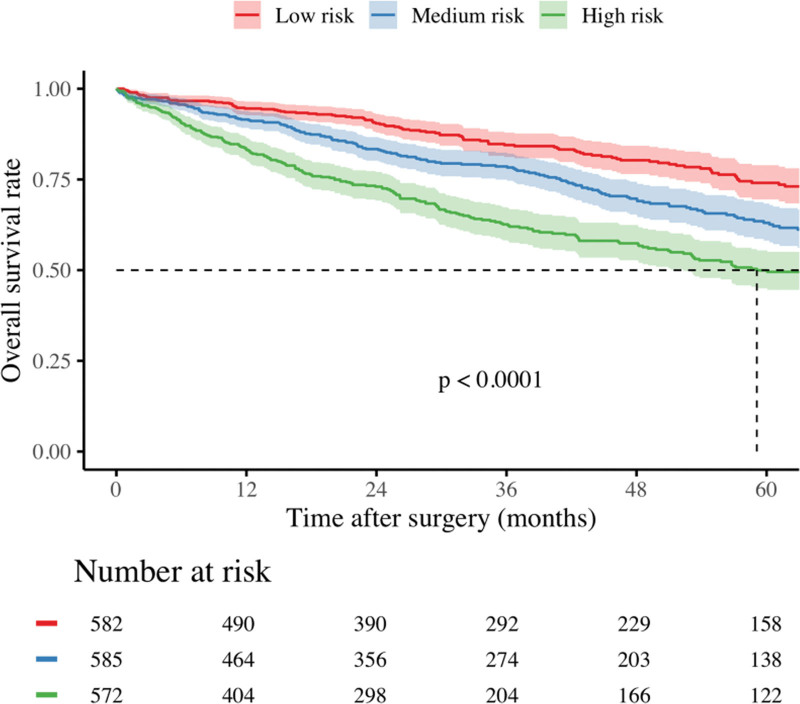
Methods: Patients undergoing curative-intent hepatectomy for HCC (2000-2023) were classified as R, BR1, and BR2 using the original BR and a novel TBS-BR category. The TBS-BR category replaces BR's categorical tumor morphology factors with the continuous TBS (TBS² = [maximum tumor diameter]² + [number of tumors]²). Multivariable analysis identified oncologic, morphometric, and patient-level factors associated with OS, which were incorporated into an online predictive tool.
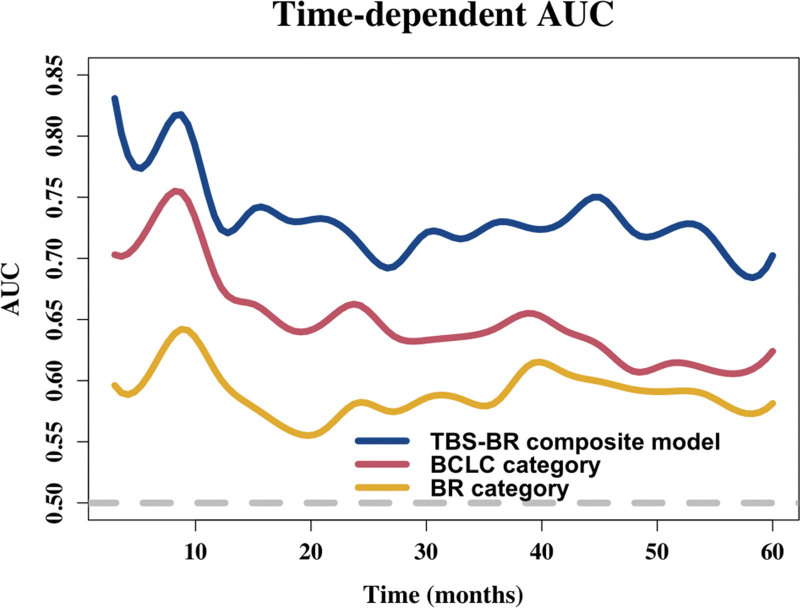
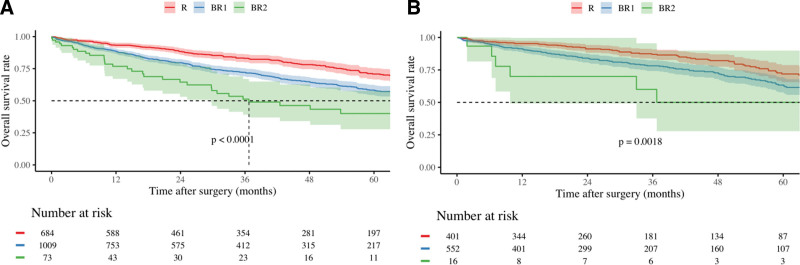
Results: Among 1766 patients, the original BR category grouped 1504 (85.2%) as R, 249 (14.1%) as BR1, and 13 (0.7%) as BR2. Utilizing the TBS-BR category, patients were reclassified as TBS-BR R (n = 684, 38.7%), BR1 (n = 1009, 57.1%), and BR2 (n = 73, 4.1%). Both the original and TBS-BR categories correlated with 5-year OS (original: 65.1%, 48.2%, 46.4%; TBS-BR: 70.8%, 58.3%, 40.0%; P < 0.001 for both; area under the curve: 0.54 vs 0.58). On multivariable analysis, TBS-BR1 (hazard ratio [HR]: 1.59 [1.20-2.09]; P = 0.001), TBS-BR2 (HR: 2.45 [1.47-4.07]; P < 0.001, reference: TBS-BR R), American Society of Anesthesiologists (ASA) class >2 (HR: 1.40 [1.09-1.80]; P = 0.007), albumin-bilirubin (ALBI) score (HR: 1.51 [1.21-1.88]; P < 0.001), and log α-fetoprotein (AFP) (HR: 1.07 [1.03-1.11]; P < 0.001) were independently associated with OS. A TBS-BR composite model based on these factors (TBS-BR category, ASA class, ALBI score, and log AFP) was developed and made available online (https://makbn.shinyapps.io/BRHCC/). The model's area under the receiver operating characteristic at 5 years (0.70) outperformed both the original BR (0.57) and Barcelona Clinic Liver Cancer classification (0.64).
Conclusions: The TBS-BR composite model, integrating tumor morphology (TBS), tumor biology (log AFP), overall physical status (ASA class), and liver function (ALBI score) demonstrated superior predictive accuracy for OS compared with the original BR and Barcelona Clinic Liver Cancer classifications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


