{"title":"Comparing Methods for Classification of Hospital Visits in the Danish National Patient Registry (DNPR): DNPR3 Versus DNPR2.","authors":"Kirsten Skjærbæk Duch, Bergur Magnussen, Flemming Skjøth, Rasmus Westermann, Lene Wohlfahrt Dreyer","doi":"10.2147/CLEP.S499822","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The Danish National Patient Registry (DNPR) is a central source of information on hospital contacts for the Danish population and is a key data source for health-related Danish registry studies. The data structure of DNPR was updated from DNPR2 to DNPR3 in 2019, where a key patient-type variable for classification of inpatient, outpatient, or emergency wards was removed. This affects how hospital contacts can be defined and compared across different calendar years.</p><p><strong>Aim: </strong>To present and compare different algorithms to determine the type of hospital visit (inpatient, outpatient, or emergency) for all hospital visits in Denmark from 2006 to 2021 across DNPR2 and DNPR3.</p><p><strong>Methods: </strong>The monthly number of hospital visits per 1000 citizens was presented for four different algorithms: 1) a validated approach suggested by Skjøth et al, 2) an approach suggested by the Danish Ministry of Health and Elderly, 3) the latter combined with patient type variables available in DNPR2 only, and 4) a consensus-driven algorithm introduced by Gregersen et al.</p><p><strong>Results: </strong>Using the same algorithm for DNPR2 and DNPR3 yielded the most similar results across calendar years. The least variation across calendar years was observed for the approach suggested by the Danish Ministry of Health and Elderly, whereas the validated approach suggested by Skjøth et al was more in line with the patient-type variable previously used in DNPR2. When comparing the algorithms, the main difference in the number of hospital visits was observed for inpatient and emergency visits.</p><p><strong>Conclusion: </strong>We recommend using the same algorithm across DNPR2 and DNPR3. The choice of algorithm should be based on the disease or patient group being studied and by considering how the approaches reflect reality and need in the actual study. We recommend the algorithm suggested by Skjøth et al for the specific clinical situations presented in this study.</p>","PeriodicalId":10362,"journal":{"name":"Clinical Epidemiology","volume":"17 ","pages":"277-285"},"PeriodicalIF":3.2000,"publicationDate":"2025-03-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11934881/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Epidemiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/CLEP.S499822","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
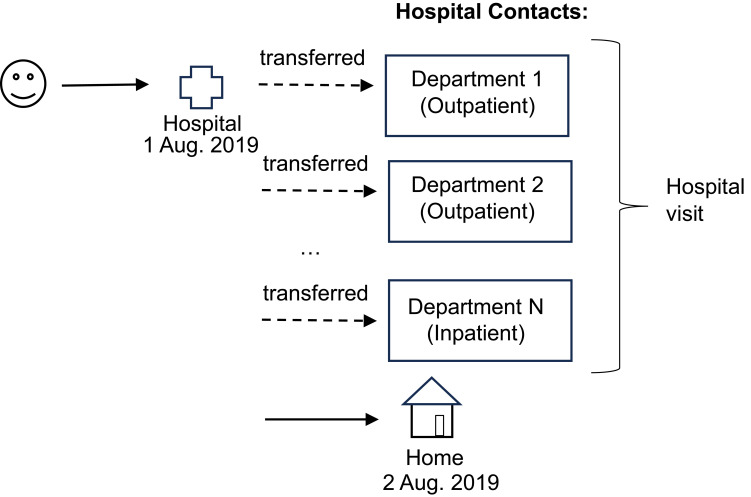
Background: The Danish National Patient Registry (DNPR) is a central source of information on hospital contacts for the Danish population and is a key data source for health-related Danish registry studies. The data structure of DNPR was updated from DNPR2 to DNPR3 in 2019, where a key patient-type variable for classification of inpatient, outpatient, or emergency wards was removed. This affects how hospital contacts can be defined and compared across different calendar years.
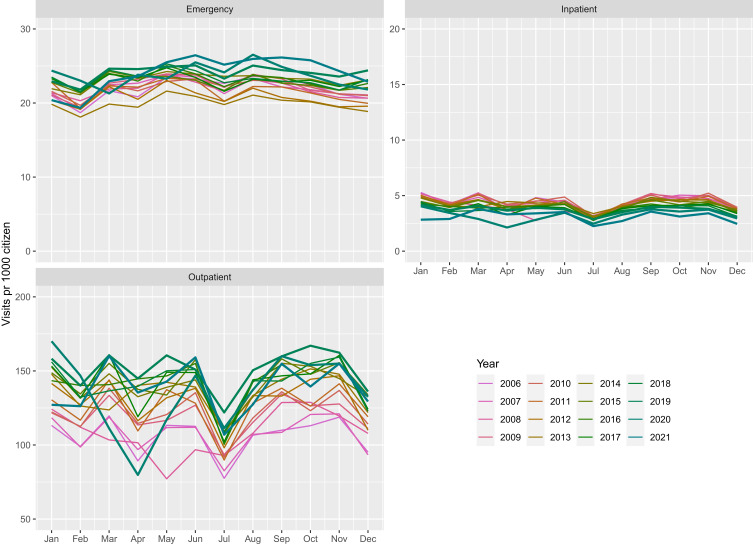
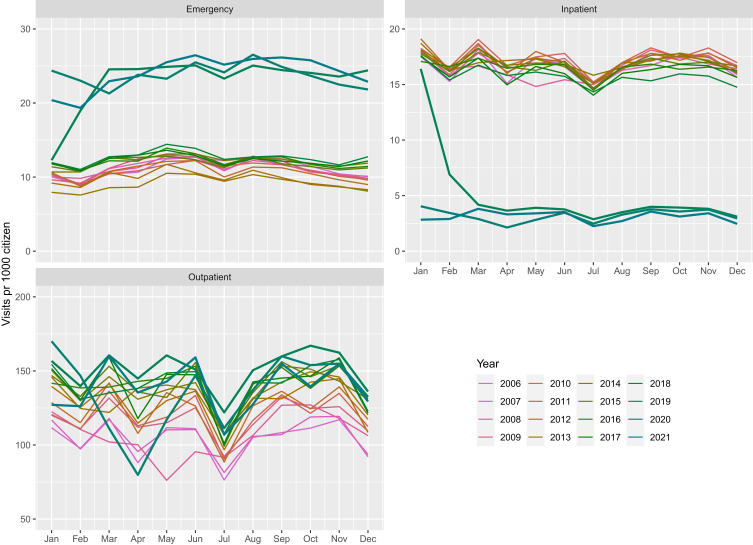
Aim: To present and compare different algorithms to determine the type of hospital visit (inpatient, outpatient, or emergency) for all hospital visits in Denmark from 2006 to 2021 across DNPR2 and DNPR3.
Methods: The monthly number of hospital visits per 1000 citizens was presented for four different algorithms: 1) a validated approach suggested by Skjøth et al, 2) an approach suggested by the Danish Ministry of Health and Elderly, 3) the latter combined with patient type variables available in DNPR2 only, and 4) a consensus-driven algorithm introduced by Gregersen et al.
Results: Using the same algorithm for DNPR2 and DNPR3 yielded the most similar results across calendar years. The least variation across calendar years was observed for the approach suggested by the Danish Ministry of Health and Elderly, whereas the validated approach suggested by Skjøth et al was more in line with the patient-type variable previously used in DNPR2. When comparing the algorithms, the main difference in the number of hospital visits was observed for inpatient and emergency visits.
Conclusion: We recommend using the same algorithm across DNPR2 and DNPR3. The choice of algorithm should be based on the disease or patient group being studied and by considering how the approaches reflect reality and need in the actual study. We recommend the algorithm suggested by Skjøth et al for the specific clinical situations presented in this study.
期刊介绍:
Clinical Epidemiology is an international, peer reviewed, open access journal. Clinical Epidemiology focuses on the application of epidemiological principles and questions relating to patients and clinical care in terms of prevention, diagnosis, prognosis, and treatment.
Clinical Epidemiology welcomes papers covering these topics in form of original research and systematic reviews.
Clinical Epidemiology has a special interest in international electronic medical patient records and other routine health care data, especially as applied to safety of medical interventions, clinical utility of diagnostic procedures, understanding short- and long-term clinical course of diseases, clinical epidemiological and biostatistical methods, and systematic reviews.
When considering submission of a paper utilizing publicly-available data, authors should ensure that such studies add significantly to the body of knowledge and that they use appropriate validated methods for identifying health outcomes.
The journal has launched special series describing existing data sources for clinical epidemiology, international health care systems and validation studies of algorithms based on databases and registries.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


