{"title":"Comparison of Laryngoscope-Guided Insertion and Standard Blind Insertion of the Laryngeal Mask Airway: A Systematic Review and Meta-Analysis.","authors":"Zhihao Zheng, Haibo Li, Congcong Dai, Liwei Bi, Wei Sun, Miao Yu, Zhanfei Hu, Xiaodong Liang","doi":"10.1155/anrp/1224567","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> The insertion of a laryngeal mask airway (LMA) using a laryngoscope-guided technique has produced inconsistent outcomes. The use of laryngoscope guidance in facilitating LMA insertion needs further investigation. This meta-analysis compared its effectiveness and safety against standard blind insertion. <b>Method:</b> We systematically searched PubMed, Cochrane Library, Web of Science, and Ovid Medline for randomized controlled trials comparing laryngoscope-guided (Group L) and blind LMA insertion (Group B). The primary outcome measured was fiberoptic staging. The secondary outcomes included oropharyngeal leak pressure (OLP), insertion time, success rate on the first attempt, and the incidence of postoperative sore throat and blood staining. <b>Results:</b> Nine RCTs (1016 patients) were analyzed. The fiberoptic staging in Group L was found to be significantly higher than that in Group B (RR = 1.54; 95% CI: 1.14-2.08; <i>p</i>=0.005). In addition, the OLP of Group L is significantly higher than that of Group B (MD = 2.10 cmH<sub>2</sub>O; 95% CI: 0.38 cmH<sub>2</sub>O-3.83 cmH<sub>2</sub>O; <i>p</i>=0.02). The success rate for the first attempt was also higher in Group L (RR = 1.14; 95% CI: 1.06-1.22; <i>p</i>=0.0005). The insertion time (MD = 3.92 s; 95% CI: -6.69 s-14.52 s; <i>p</i>=0.47), the incidence of sore throat (RR = 0.90; 95% CI: 0.50-1.65; <i>p</i>=0.74), and the incidence of blood staining (RR = 1.19; 95% CI: 0.29-4.79; <i>p</i>=0.81) did not demonstrate statistically significant differences. <b>Conclusion:</b> The use of LMA with laryngoscope guidance may improve fiberoptic staging and OLP and increase the success rate of first-attempt insertion, without significantly raising the incidence of sore throat or blood staining in anesthetized patients.</p>","PeriodicalId":7834,"journal":{"name":"Anesthesiology Research and Practice","volume":"2025 ","pages":"1224567"},"PeriodicalIF":1.3000,"publicationDate":"2025-03-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11936533/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesiology Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/anrp/1224567","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
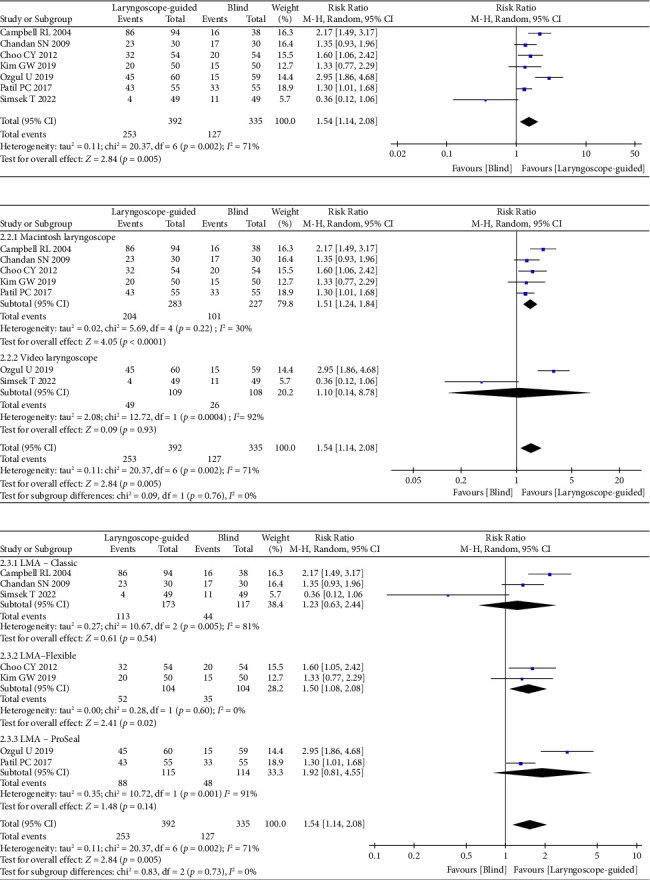
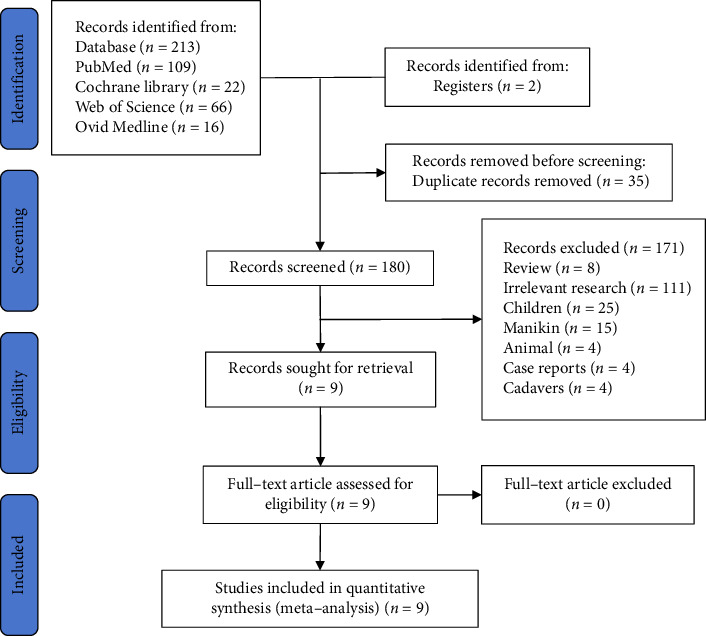
Background: The insertion of a laryngeal mask airway (LMA) using a laryngoscope-guided technique has produced inconsistent outcomes. The use of laryngoscope guidance in facilitating LMA insertion needs further investigation. This meta-analysis compared its effectiveness and safety against standard blind insertion. Method: We systematically searched PubMed, Cochrane Library, Web of Science, and Ovid Medline for randomized controlled trials comparing laryngoscope-guided (Group L) and blind LMA insertion (Group B). The primary outcome measured was fiberoptic staging. The secondary outcomes included oropharyngeal leak pressure (OLP), insertion time, success rate on the first attempt, and the incidence of postoperative sore throat and blood staining. Results: Nine RCTs (1016 patients) were analyzed. The fiberoptic staging in Group L was found to be significantly higher than that in Group B (RR = 1.54; 95% CI: 1.14-2.08; p=0.005). In addition, the OLP of Group L is significantly higher than that of Group B (MD = 2.10 cmH2O; 95% CI: 0.38 cmH2O-3.83 cmH2O; p=0.02). The success rate for the first attempt was also higher in Group L (RR = 1.14; 95% CI: 1.06-1.22; p=0.0005). The insertion time (MD = 3.92 s; 95% CI: -6.69 s-14.52 s; p=0.47), the incidence of sore throat (RR = 0.90; 95% CI: 0.50-1.65; p=0.74), and the incidence of blood staining (RR = 1.19; 95% CI: 0.29-4.79; p=0.81) did not demonstrate statistically significant differences. Conclusion: The use of LMA with laryngoscope guidance may improve fiberoptic staging and OLP and increase the success rate of first-attempt insertion, without significantly raising the incidence of sore throat or blood staining in anesthetized patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


