Daniel H Solomon, Misti Paudel, Shravani Chitineni, Ana Fernandes, Tammy Pham, Shreya Billa, Chio Yokose, Kiara Tan, Julien J Dedier, Maureen D Dubreuil, John D Fitzgerald, Sally L Hodder, Tuhina Neogi, Michael H Pillinger, Kevin R Riggs, Kenneth G Saag, Paul G Shekelle, Zoe Tseng, Michael Toprover, David S Wei, Michael J Barry, Hyon K Choi
{"title":"The Design of a Randomized Controlled Active Comparator Strategy Trial for Gout: Treat to Target Serum Urate Versus Treat to Avoid Symptoms.","authors":"Daniel H Solomon, Misti Paudel, Shravani Chitineni, Ana Fernandes, Tammy Pham, Shreya Billa, Chio Yokose, Kiara Tan, Julien J Dedier, Maureen D Dubreuil, John D Fitzgerald, Sally L Hodder, Tuhina Neogi, Michael H Pillinger, Kevin R Riggs, Kenneth G Saag, Paul G Shekelle, Zoe Tseng, Michael Toprover, David S Wei, Michael J Barry, Hyon K Choi","doi":"10.1002/acr2.70012","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Controversy persists regarding the optimal management of gout in routine primary care. There is a lack of clarity on whether treating to a target serum urate (TTT-SU) versus treating to avoid symptoms (TTASx) is more effective.</p><p><strong>Methods: </strong>We designed a randomized controlled comparative effectiveness trial aimed at patients in primary care who have known gout, have elevated SU levels, and had at least one flare in the previous 12 months. The trial was designed to be pragmatic and incorporated structured input from primary care physicians, rheumatologists, and patients. The TTASx strategy group will receive weeklong courses of typical therapies for gout flares, such as colchicine, naproxen, or an oral glucocorticoid. The TTT-SU strategy group will receive urate-lowering therapy (primarily allopurinol) with dose titration to maintain an SU level <6 mg/dL, colchicine (or naproxen) prophylaxis for the first six months of urate-lowering therapy, and access to the same flare therapies as the TTASx group. Two clinicians (nurses or physicians) per site will be trained in each strategy to manage the patients in each arm without contamination. Gout flares are the primary outcome and are assessed every two weeks by trained study staff masked to treatment assignment using a validated questionnaire. The secondary outcome is quality of life. Blood pressure control, kidney function, glycemic control, and coronary atherosclerosis are exploratory secondary outcomes.</p><p><strong>Results: </strong>Several sites have started prescreening using automated search strategies in their patients' electronic health records. Of the first 1,381 patients found in primary care practices with a history of gout, 691 patients (50%) passed prescreening checks. These potentially eligible participants have a median age of 67 years, 85% are men, median SU levels are 7.2 mg/dL, and 18% are taking low dosages of allopurinol. These patients have been targeted for recruitment efforts that are underway now.</p><p><strong>Conclusion: </strong>This randomized controlled active comparator strategy trial will answer a key question in the treatment of patients with gout in primary care: the comparative effectiveness of TTT-SU versus TTASx in gout. Secondary and exploratory outcomes will add important information regarding the broader extra-articular and quality-of-life effects of lowering SU levels.</p>","PeriodicalId":93845,"journal":{"name":"ACR open rheumatology","volume":"7 3","pages":"e70012"},"PeriodicalIF":2.8000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11932158/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACR open rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/acr2.70012","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Controversy persists regarding the optimal management of gout in routine primary care. There is a lack of clarity on whether treating to a target serum urate (TTT-SU) versus treating to avoid symptoms (TTASx) is more effective.
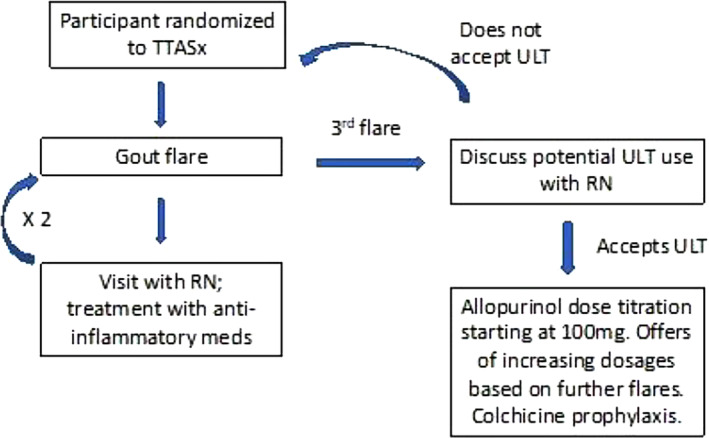
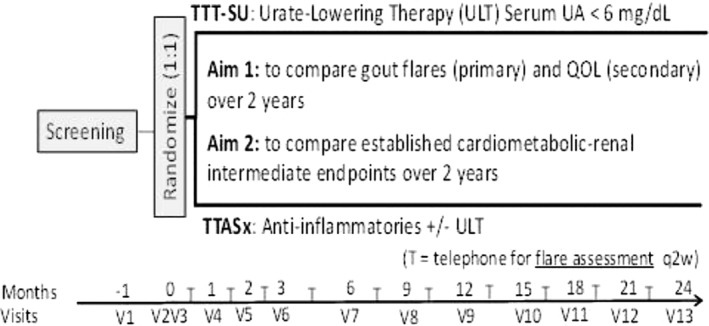
Methods: We designed a randomized controlled comparative effectiveness trial aimed at patients in primary care who have known gout, have elevated SU levels, and had at least one flare in the previous 12 months. The trial was designed to be pragmatic and incorporated structured input from primary care physicians, rheumatologists, and patients. The TTASx strategy group will receive weeklong courses of typical therapies for gout flares, such as colchicine, naproxen, or an oral glucocorticoid. The TTT-SU strategy group will receive urate-lowering therapy (primarily allopurinol) with dose titration to maintain an SU level <6 mg/dL, colchicine (or naproxen) prophylaxis for the first six months of urate-lowering therapy, and access to the same flare therapies as the TTASx group. Two clinicians (nurses or physicians) per site will be trained in each strategy to manage the patients in each arm without contamination. Gout flares are the primary outcome and are assessed every two weeks by trained study staff masked to treatment assignment using a validated questionnaire. The secondary outcome is quality of life. Blood pressure control, kidney function, glycemic control, and coronary atherosclerosis are exploratory secondary outcomes.
Results: Several sites have started prescreening using automated search strategies in their patients' electronic health records. Of the first 1,381 patients found in primary care practices with a history of gout, 691 patients (50%) passed prescreening checks. These potentially eligible participants have a median age of 67 years, 85% are men, median SU levels are 7.2 mg/dL, and 18% are taking low dosages of allopurinol. These patients have been targeted for recruitment efforts that are underway now.
Conclusion: This randomized controlled active comparator strategy trial will answer a key question in the treatment of patients with gout in primary care: the comparative effectiveness of TTT-SU versus TTASx in gout. Secondary and exploratory outcomes will add important information regarding the broader extra-articular and quality-of-life effects of lowering SU levels.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


