Screening for pre-eclampsia using pregnancy-associated plasma protein-A or placental growth factor measurements in blood samples collected at 8-14 weeks' gestation.
Objectives: To assess the value of pregnancy-associated plasma protein-A (PAPP-A) in screening for preterm pre-eclampsia (PE) (delivery < 37 weeks' gestation) measured in maternal blood samples collected before 11 weeks, and to compare the screening performance of PAPP-A with that of placental growth factor (PlGF) from blood samples collected at 8-14 weeks.
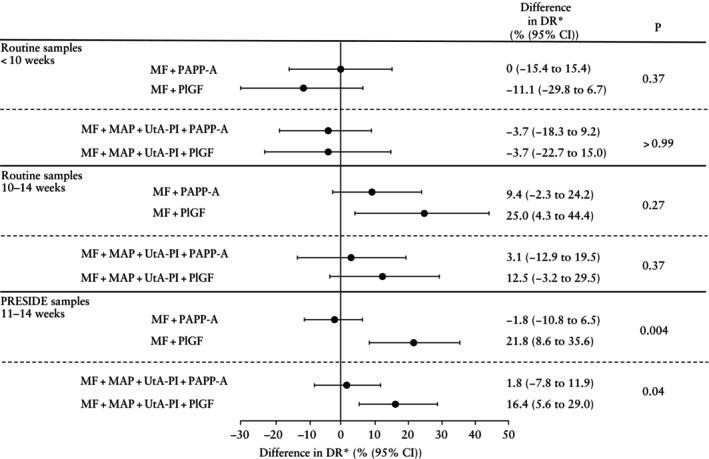
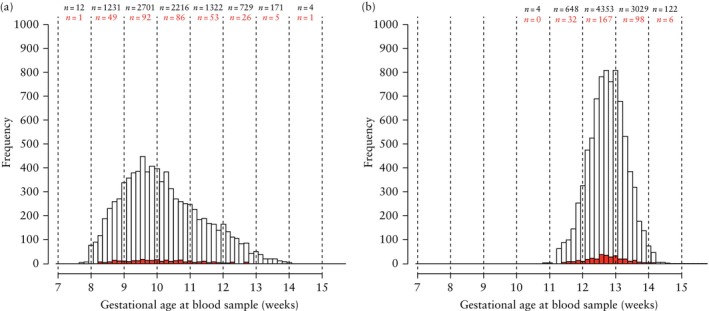
Methods: This study analyzed data from women who participated in the PRESIDE (Pre-eclampsia Screening in Denmark) study, a prospective, non-interventional multicenter study investigating the predictive performance of the Fetal Medicine Foundation first-trimester screening algorithm for PE in a Danish population. As part of combined first-trimester screening, a routine blood sample was collected at 8-14 weeks' gestation and PAPP-A was measured. Excess serum was stored at -80°C and analyzed for PlGF in batches after delivery. Most women in the PRESIDE study had an extra blood sample collected at the time of the first-trimester scan at 11-14 weeks, which was also analyzed for PlGF and PAPP-A in batches after all the participants had delivered. Screening performance was assessed in terms of the detection rate at a 10% screen-positive rate (SPR) for a combination of PAPP-A or PlGF with maternal factors alone and for a combination of each of these biomarkers with maternal factors, mean arterial pressure (MAP) and uterine artery pulsatility index (UtA-PI).
Results: The study population comprised 8386 women who had a routine combined first-trimester aneuploidy screening blood sample collected at 8-14 weeks' gestation. In pregnancies that developed preterm PE, the median PAPP-A multiples of the median from routine blood samples were 0.78 (95% CI, 0.67-0.90) before 10 weeks, 0.80 (95% CI, 0.58-1.10) at 10 weeks and 0.64 (95% CI, 0.53-0.78) at 11-14 weeks. In women with samples collected before 10 weeks, there was no significant improvement in the detection rate of preterm PE when PAPP-A or PlGF was combined with maternal factors alone or when combined with maternal factors, MAP and UtA-PI. In routine samples collected at or after 10 weeks, PAPP-A only increased the detection rate of preterm PE slightly. However, PlGF in samples collected at or after 10 weeks increased the detection rate from 31.3% (95% CI, 16.1-50.0%) to 56.3% (95% CI, 37.7-73.6%) at a 10% SPR, i.e. an increase in the detection rate of 25.0% (95% CI, 4.3-44.4%), when combined with maternal factors alone. When PlGF collected from the PRESIDE sample at 11-14 weeks was combined with maternal factors, MAP and UtA-PI, there was an increase in the detection rate from 50.9% (95% CI, 37.1-64.6%) to 67.3% (95% CI, 53.3-79.3%), i.e. an increase of 16.4% (95% CI, 5.6-29.0%) at a 10% SPR.
期刊介绍:
Ultrasound in Obstetrics & Gynecology (UOG) is the official journal of the International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) and is considered the foremost international peer-reviewed journal in the field. It publishes cutting-edge research that is highly relevant to clinical practice, which includes guidelines, expert commentaries, consensus statements, original articles, and systematic reviews. UOG is widely recognized and included in prominent abstract and indexing databases such as Index Medicus and Current Contents.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


