{"title":"Immune Checkpoint Inhibitor-induced Myocarditis: A Case Report of Complete Heart Block and Challenges in a Patient on Pembrolizumab.","authors":"Viraj Panchal, Elina Momin, Shubhika Jain, Anaiya Singh, Guntas Ghuman, Vijaywant Brar","doi":"10.19102/icrm.2025.16033","DOIUrl":null,"url":null,"abstract":"<p><p>Immune checkpoint inhibitors (ICIs) have revolutionized cancer treatment by modulating immune responses, leading to enhanced anti-tumor activity. ICIs, including agents targeting cytotoxic T-lymphocyte antigen 4, programmed cell death 1, and programmed cell death ligand, are now widely used in various malignancies, either as monotherapy or in combination with chemotherapy, radiotherapy, or targeted therapies. However, ICIs are associated with immune-related adverse events, affecting multiple organ systems, with myocarditis emerging as a rare but potentially fatal complication. We present a 67-year-old man with a history of prostate and renal cell carcinoma treated with pembrolizumab and lenvatinib, who developed myocarditis secondary to ICI therapy. The patient initially presented with generalized fatigue and bradycardia, later progressing to more severe symptoms, including sinus bradycardia and elevated troponin levels. An electrocardiogram revealed a sinus rhythm with first-degree atrioventricular block, non-specific intraventricular conduction delay, and elevated high-sensitivity troponin levels progressively increasing to 50,000 pg/mL. A comprehensive diagnostic workup ruled out ischemic causes, leading to the diagnosis of ICI-induced myocarditis. The patient was treated with high-dose corticosteroids, intravenous immunoglobulin, and temporary pacemaker insertion, resulting in clinical improvement. This case highlights the need for vigilance and prompt intervention in patients receiving ICI therapy, as early recognition and treatment of myocarditis are crucial to optimizing patient outcomes in this high-risk population.</p>","PeriodicalId":36299,"journal":{"name":"Journal of Innovations in Cardiac Rhythm Management","volume":"16 3","pages":"6215-6219"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11927601/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Innovations in Cardiac Rhythm Management","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.19102/icrm.2025.16033","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
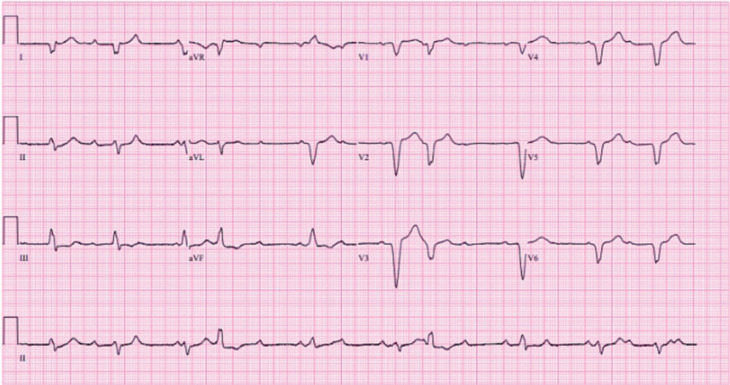
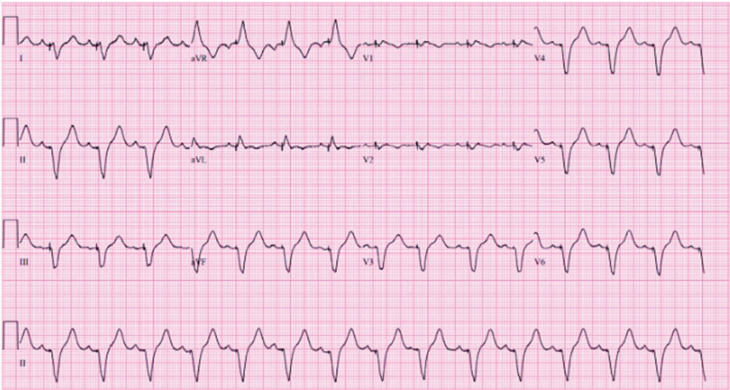
Immune checkpoint inhibitors (ICIs) have revolutionized cancer treatment by modulating immune responses, leading to enhanced anti-tumor activity. ICIs, including agents targeting cytotoxic T-lymphocyte antigen 4, programmed cell death 1, and programmed cell death ligand, are now widely used in various malignancies, either as monotherapy or in combination with chemotherapy, radiotherapy, or targeted therapies. However, ICIs are associated with immune-related adverse events, affecting multiple organ systems, with myocarditis emerging as a rare but potentially fatal complication. We present a 67-year-old man with a history of prostate and renal cell carcinoma treated with pembrolizumab and lenvatinib, who developed myocarditis secondary to ICI therapy. The patient initially presented with generalized fatigue and bradycardia, later progressing to more severe symptoms, including sinus bradycardia and elevated troponin levels. An electrocardiogram revealed a sinus rhythm with first-degree atrioventricular block, non-specific intraventricular conduction delay, and elevated high-sensitivity troponin levels progressively increasing to 50,000 pg/mL. A comprehensive diagnostic workup ruled out ischemic causes, leading to the diagnosis of ICI-induced myocarditis. The patient was treated with high-dose corticosteroids, intravenous immunoglobulin, and temporary pacemaker insertion, resulting in clinical improvement. This case highlights the need for vigilance and prompt intervention in patients receiving ICI therapy, as early recognition and treatment of myocarditis are crucial to optimizing patient outcomes in this high-risk population.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


