Jaclyn K Schwartz, Emily A Kringle, Suzanne Perea Burns, Catherine R Hoyt, Kelly M Harris, Sami Tayeb
{"title":"Cardiovascular Outcomes, Health-Promoting Behaviors, and Social Determinants: Structural Racism and the Behavioral Risk Factor Surveillance System.","authors":"Jaclyn K Schwartz, Emily A Kringle, Suzanne Perea Burns, Catherine R Hoyt, Kelly M Harris, Sami Tayeb","doi":"10.1089/heq.2023.0203","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Cardiovascular disease disproportionately affects historically marginalized populations in the United States. This study explored disparities in cardiovascular health outcomes, social determinants of health, and health-promoting behaviors across racial and ethnic groups.</p><p><strong>Methods: </strong>Using data from the 2019 Behavioral Risk Factor Surveillance System, we conducted a descriptive analysis of cardiovascular conditions and diabetes, social determinants of health, and health-promoting behaviors across eight racial/ethnic categories.</p><p><strong>Results: </strong>Historically marginalized groups had higher rates of cardiovascular conditions and greater barriers to health care access. However, these groups often demonstrated equal or higher rates of engagement in health-promoting behaviors compared with White adults. For example, Black adults had the highest hypertension prevalence (41%) despite having the highest rates of blood pressure management behaviors.</p><p><strong>Discussion: </strong>The persistence of health disparities despite equivalent health-promoting behaviors suggests a significant influence of structural factors like racism. Critical examination using Quantitative Critical Theory revealed potential biases in measurement tools and data categorization that may perpetuate inequities.</p><p><strong>Health equity implications: </strong>Findings underscore the need for equity-focused research approaches that explicitly address structural racism. Future studies should prioritize culturally relevant measures, clinically meaningful outcomes, and active involvement of researchers from marginalized communities to advance cardiovascular health equity.</p>","PeriodicalId":36602,"journal":{"name":"Health Equity","volume":"8 1","pages":"707-719"},"PeriodicalIF":2.5000,"publicationDate":"2024-10-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11499743/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Equity","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1089/heq.2023.0203","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Cardiovascular disease disproportionately affects historically marginalized populations in the United States. This study explored disparities in cardiovascular health outcomes, social determinants of health, and health-promoting behaviors across racial and ethnic groups.
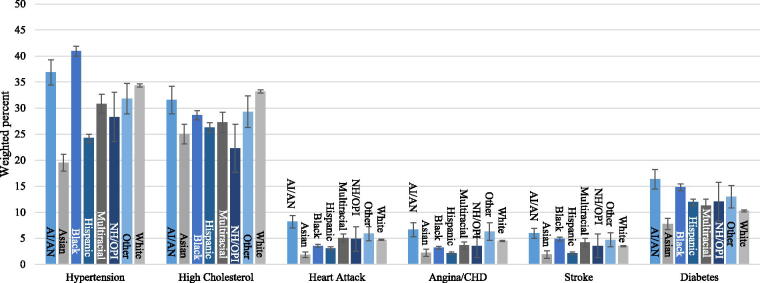
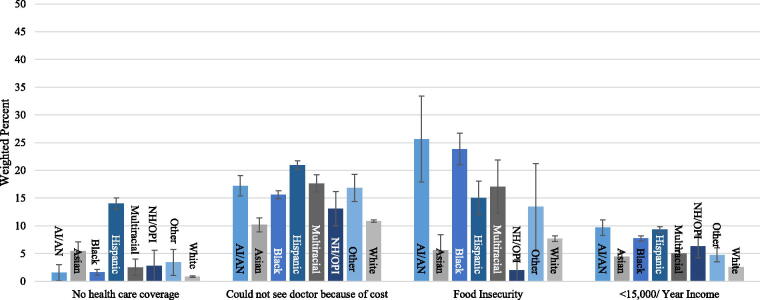
Methods: Using data from the 2019 Behavioral Risk Factor Surveillance System, we conducted a descriptive analysis of cardiovascular conditions and diabetes, social determinants of health, and health-promoting behaviors across eight racial/ethnic categories.
Results: Historically marginalized groups had higher rates of cardiovascular conditions and greater barriers to health care access. However, these groups often demonstrated equal or higher rates of engagement in health-promoting behaviors compared with White adults. For example, Black adults had the highest hypertension prevalence (41%) despite having the highest rates of blood pressure management behaviors.
Discussion: The persistence of health disparities despite equivalent health-promoting behaviors suggests a significant influence of structural factors like racism. Critical examination using Quantitative Critical Theory revealed potential biases in measurement tools and data categorization that may perpetuate inequities.
Health equity implications: Findings underscore the need for equity-focused research approaches that explicitly address structural racism. Future studies should prioritize culturally relevant measures, clinically meaningful outcomes, and active involvement of researchers from marginalized communities to advance cardiovascular health equity.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


