Effects of Noninvasive Respiratory Support on Ventilation Distribution During Spontaneous Breathing Sedation in Preschool/School-Aged Children: An Electrical Impedance Tomography Study.
Giovanna Chidini, Tiziana Marchesi, Stefano Scalia Catenacci, Gaetano Florio, Giorgio Conti, Stefano Lanni, Giovanni Filocamo, Francesca Patria, Marta Guerrini, Gregorio Milani, Giacomo Grasselli
{"title":"Effects of Noninvasive Respiratory Support on Ventilation Distribution During Spontaneous Breathing Sedation in Preschool/School-Aged Children: An Electrical Impedance Tomography Study.","authors":"Giovanna Chidini, Tiziana Marchesi, Stefano Scalia Catenacci, Gaetano Florio, Giorgio Conti, Stefano Lanni, Giovanni Filocamo, Francesca Patria, Marta Guerrini, Gregorio Milani, Giacomo Grasselli","doi":"10.1111/pan.15098","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Procedural sedation interferes with respiratory dynamics in pediatric patients. It reduces lung compliance, causing the closing volume to exceed the functional residual capacity, which can result in airway collapse, atelectasis, and periods of silent desaturation.</p><p><strong>Aim: </strong>Aims of the study were to clarify the impact of intravenous propofol sedation on ventilation distribution and to evaluate the potential benefits of noninvasive respiratory support (NRS) in restoring the original ventilation distribution pattern by applying the electrical impedance tomography technology.</p><p><strong>Methods: </strong>Single-center physiological randomized crossover study comparing two 20-min steps of NRS delivered as continuous positive airway pressure (CPAP) and noninvasive ventilation (NIV) at different time points: (1) spontaneous breathing (SB-1); (2) spontaneous breathing during sedation (SB-2); (3) CPAP during sedation; (4) NIV during sedation; (5) spontaneous breathing after sedation discontinuation (SB-3). Primary endpoint was regional ventilation delay 40% (RVD40%). Secondary outcomes were global index (GI), end-expiratory lung impedance (EELI), and center of ventilation (CoV).</p><p><strong>Results: </strong>Thirteen children were enrolled. RVD40% increased during SB-2 compared to SB-1 (p = 0.014). NIV was effective in reducing it compared to CPAP (p = 0.009) and SB-3 (p = 0.015). NIV was also effective in restoring ventilation homogeneity and lung volume compared to SB-2 by decreasing GI (p = 0.035) and restoring EELI (p = 0.002). During NIV, the center of ventilation increased compared to SB-1 (p = 0.001), SB-2 (p = 0.004), and CPAP (p = 0.004), suggesting that ventilation was shifted toward the ventral areas of the lungs. On the other hand, CPAP was not effective in restoring RVD40, GI, and EELI to SB1 values following the induction of intravenous anesthesia with propofol at SB-2.</p><p><strong>Conclusions: </strong>In this specific ventilatory setting, spontaneous breathing sedation resulted in enhanced ventilation inhomogeneity and a reduction in EELI that could be reversed by NIV but not by CPAP.</p><p><strong>Clinical trials registration: </strong>The trial was registered prior to patient enrollment at Clinicaltrials.gov (NCT05495477; principal investigator: Giovanna Chidini; date of registration: August 10, 2022). Consolidated Standards of Reporting Trials guidelines were followed, and the study was conducted according to the Helsinki 1964 Ethical Declaration Standard, revised in 2008.</p>","PeriodicalId":19745,"journal":{"name":"Pediatric Anesthesia","volume":" ","pages":"562-572"},"PeriodicalIF":1.7000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12149492/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Anesthesia","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/pan.15098","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/22 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Procedural sedation interferes with respiratory dynamics in pediatric patients. It reduces lung compliance, causing the closing volume to exceed the functional residual capacity, which can result in airway collapse, atelectasis, and periods of silent desaturation.
Aim: Aims of the study were to clarify the impact of intravenous propofol sedation on ventilation distribution and to evaluate the potential benefits of noninvasive respiratory support (NRS) in restoring the original ventilation distribution pattern by applying the electrical impedance tomography technology.
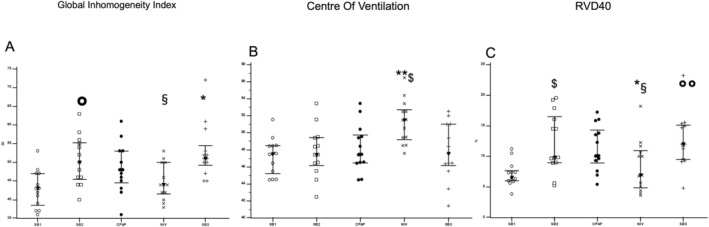
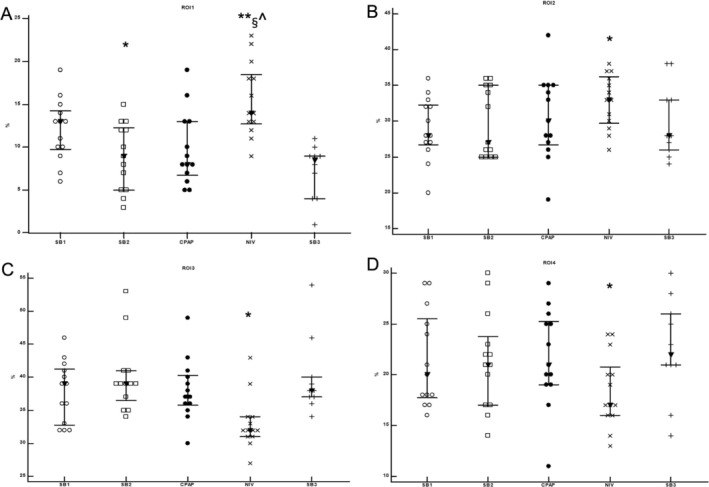
Methods: Single-center physiological randomized crossover study comparing two 20-min steps of NRS delivered as continuous positive airway pressure (CPAP) and noninvasive ventilation (NIV) at different time points: (1) spontaneous breathing (SB-1); (2) spontaneous breathing during sedation (SB-2); (3) CPAP during sedation; (4) NIV during sedation; (5) spontaneous breathing after sedation discontinuation (SB-3). Primary endpoint was regional ventilation delay 40% (RVD40%). Secondary outcomes were global index (GI), end-expiratory lung impedance (EELI), and center of ventilation (CoV).
Results: Thirteen children were enrolled. RVD40% increased during SB-2 compared to SB-1 (p = 0.014). NIV was effective in reducing it compared to CPAP (p = 0.009) and SB-3 (p = 0.015). NIV was also effective in restoring ventilation homogeneity and lung volume compared to SB-2 by decreasing GI (p = 0.035) and restoring EELI (p = 0.002). During NIV, the center of ventilation increased compared to SB-1 (p = 0.001), SB-2 (p = 0.004), and CPAP (p = 0.004), suggesting that ventilation was shifted toward the ventral areas of the lungs. On the other hand, CPAP was not effective in restoring RVD40, GI, and EELI to SB1 values following the induction of intravenous anesthesia with propofol at SB-2.
Conclusions: In this specific ventilatory setting, spontaneous breathing sedation resulted in enhanced ventilation inhomogeneity and a reduction in EELI that could be reversed by NIV but not by CPAP.
Clinical trials registration: The trial was registered prior to patient enrollment at Clinicaltrials.gov (NCT05495477; principal investigator: Giovanna Chidini; date of registration: August 10, 2022). Consolidated Standards of Reporting Trials guidelines were followed, and the study was conducted according to the Helsinki 1964 Ethical Declaration Standard, revised in 2008.
期刊介绍:
Devoted to the dissemination of research of interest and importance to practising anesthetists everywhere, the scientific and clinical content of Pediatric Anesthesia covers a wide selection of medical disciplines in all areas relevant to paediatric anaesthesia, pain management and peri-operative medicine. The International Editorial Board is supported by the Editorial Advisory Board and a team of Senior Advisors, to ensure that the journal is publishing the best work from the front line of research in the field. The journal publishes high-quality, relevant scientific and clinical research papers, reviews, commentaries, pro-con debates, historical vignettes, correspondence, case presentations and book reviews.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


