{"title":"Endotracheal Tube Size Estimation in Paediatric Patients: A Head-to-head Comparison of Accuracy Between Ultrasonography and Age-based Formula.","authors":"Archan Jayantbhai Bhut, Kalyani Nilesh Patil, Sarita Swami","doi":"10.4274/TJAR.2025.241822","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>In the paediatric population, the selection of an appropriately sized endotracheal tube (ETT) is extremely important not only to ensure adequate ventilation but also to avoid post-extubation stridor and stenosis. Conventionally, formulas based on age, height, or weight are used to determine the most appropriate size. In this study, we compared ultrasonography (USG) and age-based formula for predicting the best microcuff ETT size in paediatric patients aged 1-5 years.</p><p><strong>Methods: </strong>One hundred eighteen patients, aged 1 to 5 years, with American Society of Anesthesiologists, classifications of I or II, were included. After standard general anaesthesia protocols, the subglottic diameter was assessed by USG. Intubation was performed using ETT size according to age-based formula. The best clinical fit was determined after the leak test. The internal and external diameters of the ETTs were predicted by both methods and correlated with the best-fit ETT sizes used during the procedures using Pearson's correlation. Cohen's kappa was used for statistical agreement between two methods.</p><p><strong>Results: </strong>USG had a significantly higher correlation with the best-fit model as compared to the age-based formula, with 99.2% and 77.1% agreement rates. The best-fit ETT showed a better correlation with the USG-guided estimate (r = 0.994, <i>P</i> < 0.001). The Cohen's Kappa value of 0.986 showed a statistically significantly higher agreement between USG-guided estimate and best-fit ETT.</p><p><strong>Conclusion: </strong>USG-guided estimation of subglottic diameter is a better predictor for optimally sized microcuff ETT than the age-based formula in the paediatric age group of 1-5 years. 22% of tube changes could have been prevented with ultrasound-guidance as a primary approach for estimating ETT size.</p>","PeriodicalId":23353,"journal":{"name":"Turkish journal of anaesthesiology and reanimation","volume":"53 2","pages":"69-76"},"PeriodicalIF":0.9000,"publicationDate":"2025-03-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11931265/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Turkish journal of anaesthesiology and reanimation","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4274/TJAR.2025.241822","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: In the paediatric population, the selection of an appropriately sized endotracheal tube (ETT) is extremely important not only to ensure adequate ventilation but also to avoid post-extubation stridor and stenosis. Conventionally, formulas based on age, height, or weight are used to determine the most appropriate size. In this study, we compared ultrasonography (USG) and age-based formula for predicting the best microcuff ETT size in paediatric patients aged 1-5 years.
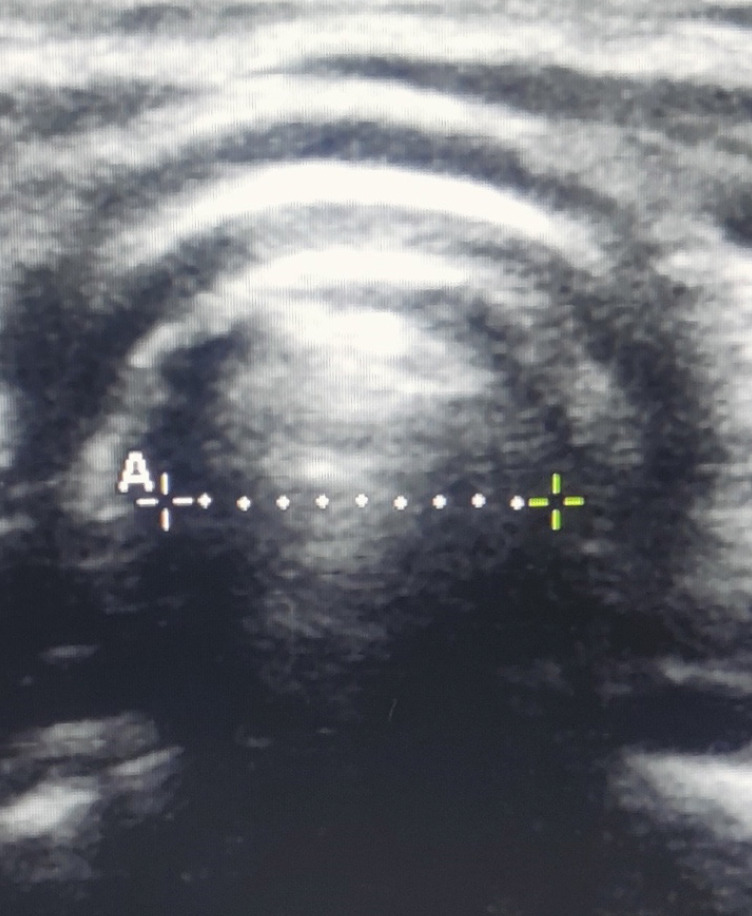
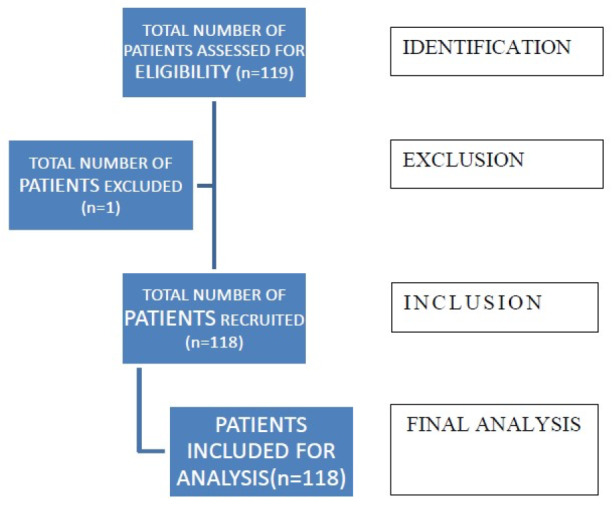
Methods: One hundred eighteen patients, aged 1 to 5 years, with American Society of Anesthesiologists, classifications of I or II, were included. After standard general anaesthesia protocols, the subglottic diameter was assessed by USG. Intubation was performed using ETT size according to age-based formula. The best clinical fit was determined after the leak test. The internal and external diameters of the ETTs were predicted by both methods and correlated with the best-fit ETT sizes used during the procedures using Pearson's correlation. Cohen's kappa was used for statistical agreement between two methods.
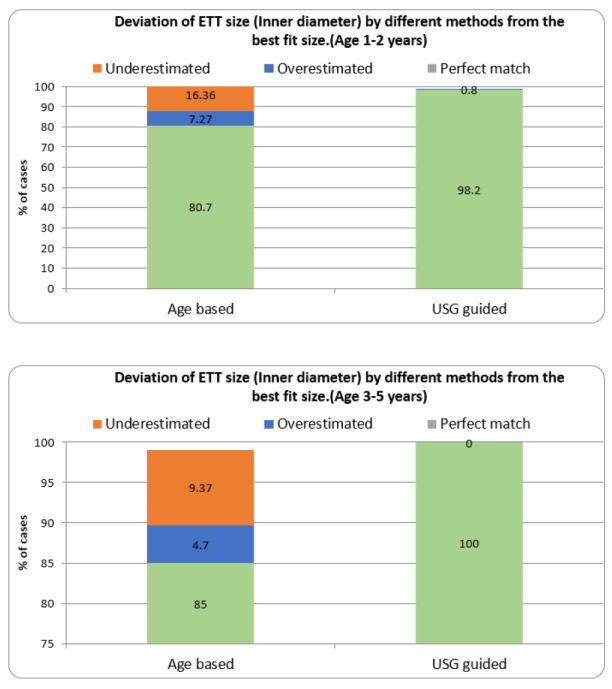
Results: USG had a significantly higher correlation with the best-fit model as compared to the age-based formula, with 99.2% and 77.1% agreement rates. The best-fit ETT showed a better correlation with the USG-guided estimate (r = 0.994, P < 0.001). The Cohen's Kappa value of 0.986 showed a statistically significantly higher agreement between USG-guided estimate and best-fit ETT.
Conclusion: USG-guided estimation of subglottic diameter is a better predictor for optimally sized microcuff ETT than the age-based formula in the paediatric age group of 1-5 years. 22% of tube changes could have been prevented with ultrasound-guidance as a primary approach for estimating ETT size.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


