{"title":"The Effect of Prone Position on Right Ventricular Functions in CARDS: Is Survival Predictable when Evaluated Through Transesophageal Echocardiography?","authors":"Dicle Birtane, Zafer Çukurova, Sinan Aşar, Damla Özmen, Gökhan Sertcakacılar, Fatma Nihan Çağlar Turhan","doi":"10.4274/TJAR.2025.241830","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To evaluate the cardiopulmonary effect during prone position (PP) on right ventricular (RV) recovery in coronavirus disease-2019 related acute respiratory distress syndrome (C-ARDS) through transesophageal echocardiography (TEE).</p><p><strong>Methods: </strong>This prospective study included 30 moderate-to-severe C-ARDS patients who were treated with PP in the first 48 h of invasive mechanical ventilation support. It was evaluated with TEE three times: before PP (T<sub>0</sub>f), the first hour of PP (T<sub>1</sub>), and the first hour of returning to the supine position (T<sub>0</sub> + 24 h) (T<sub>2</sub>) after 23 hours of PP treatment. RV end-diastolic area/left ventricular (LV) end-diastolic area (RVEDA/LVEDA), tricuspid annular plane systolic excursion (TAPSE) and LV end-systolic eccentricity index were preferred RV evaluations as primary outcomes. Pulmonary effects of PP were evaluated as a secondary outcome, including PaO<sub>2</sub>/FiO<sub>2</sub>, driving pressure (dP), static compliance (Cstat), mechanical ventilation parameters, and their association with 28-day survival. Tissue DO<sub>2</sub> was examined as a secondary outcome, and it was calculated using the measured cardiac output through TEE.</p><p><strong>Results: </strong>With the cardiopulmonary effect of PP, the decrease in RVEDA/LVEDA, the increase in TAPSE, PaO<sub>2</sub>/FiO<sub>2</sub>, and Cstat, and the decrease in dP were statistically significant (<i>P</i> < 0.05). The Cstat value associated with 28-day survival showed decreased mortality for each unit increase. The Cstat cut-off value, which was statistically significant for survival, was 37.</p><p><strong>Conclusion: </strong>PP can improve RV recovery and oxygenation, but it isn't always accompanied by increased survival. An increase in the Cstat may improve survival without the development of RV dysfunction while maintaining heart-lung interaction.</p>","PeriodicalId":23353,"journal":{"name":"Turkish journal of anaesthesiology and reanimation","volume":"53 2","pages":"53-61"},"PeriodicalIF":0.9000,"publicationDate":"2025-03-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11931261/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Turkish journal of anaesthesiology and reanimation","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4274/TJAR.2025.241830","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To evaluate the cardiopulmonary effect during prone position (PP) on right ventricular (RV) recovery in coronavirus disease-2019 related acute respiratory distress syndrome (C-ARDS) through transesophageal echocardiography (TEE).
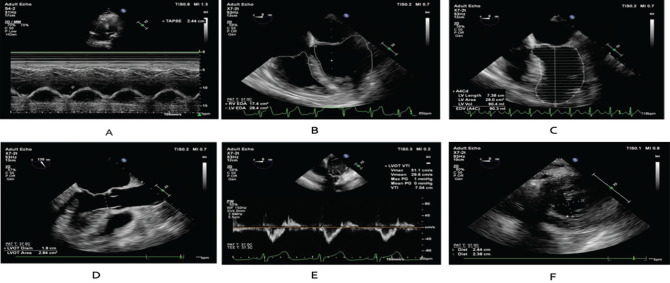
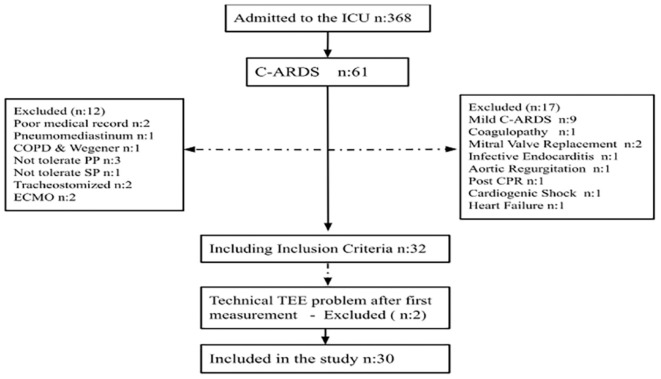
Methods: This prospective study included 30 moderate-to-severe C-ARDS patients who were treated with PP in the first 48 h of invasive mechanical ventilation support. It was evaluated with TEE three times: before PP (T0f), the first hour of PP (T1), and the first hour of returning to the supine position (T0 + 24 h) (T2) after 23 hours of PP treatment. RV end-diastolic area/left ventricular (LV) end-diastolic area (RVEDA/LVEDA), tricuspid annular plane systolic excursion (TAPSE) and LV end-systolic eccentricity index were preferred RV evaluations as primary outcomes. Pulmonary effects of PP were evaluated as a secondary outcome, including PaO2/FiO2, driving pressure (dP), static compliance (Cstat), mechanical ventilation parameters, and their association with 28-day survival. Tissue DO2 was examined as a secondary outcome, and it was calculated using the measured cardiac output through TEE.
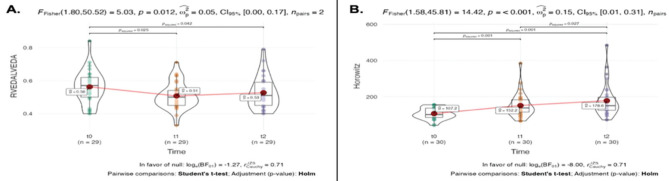
Results: With the cardiopulmonary effect of PP, the decrease in RVEDA/LVEDA, the increase in TAPSE, PaO2/FiO2, and Cstat, and the decrease in dP were statistically significant (P < 0.05). The Cstat value associated with 28-day survival showed decreased mortality for each unit increase. The Cstat cut-off value, which was statistically significant for survival, was 37.
Conclusion: PP can improve RV recovery and oxygenation, but it isn't always accompanied by increased survival. An increase in the Cstat may improve survival without the development of RV dysfunction while maintaining heart-lung interaction.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


