{"title":"Effect of primary health care on hospitalizations: health services analysis based on Estonian data.","authors":"Kaija Kasekamp, Andres Võrk, Ruth Kalda","doi":"10.1017/S1463423625000222","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>This study aims to assess the effect of primary health care (PHC) service provision continuity on inpatient admissions for people with chronic diseases in Estonia.</p><p><strong>Background: </strong>Non-communicable diseases (NCDs) were collectively responsible for more than 7 out of 10 deaths worldwide in 2019. As the burden of NCDs increases, PHC has an increased role of coordinating care management. High-performing PHC can reduce unnecessary hospitalizations. Estonia has a strong PHC system focusing on multidisciplinary care. Yet it has not been evaluated for its effect on hospitalizations. Therefore, it is imperative to evaluate PHC continuity to improve care for NCD patients.</p><p><strong>Methods: </strong>This study used routinely collected electronic medical billing data of the Estonian population aged 15 years or older from 2005 to 2020 identifying patients with seven ambulatory care sensitive chronic (ACSC) conditions. We developed an indicator to describe the continuity of PHC. Charlson Comorbidity Index (CCI) was used to assess the impact of comorbidities and we controlled the patient's age, gender, county of residency and socio-economic status. We estimated multilevel logistic regression models with family doctor patient list random effects to assess how the odds of hospitalization depend on continuity of care, allowing for confounders.</p><p><strong>Findings: </strong>We identified that 45% of the adult Estonian population had at least one of the target diagnoses. Among the target population, 96% had contact with their PHC providers. We found that there is a non-linear relationship between PHC continuity and patient outcomes. Any contact with PHC provider during the past 5 years decreases odds for hospitalization, but hospitalization risk is higher for people who are elderly and have higher CCI score. We found that after accounting for patient characteristics, differences among patient lists minimally impact outcomes. Further research should explore policies to better support family doctors in reducing hospitalizations for chronic patients.</p>","PeriodicalId":74493,"journal":{"name":"Primary health care research & development","volume":"26 ","pages":"e29"},"PeriodicalIF":1.7000,"publicationDate":"2025-03-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11955538/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Primary health care research & development","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1017/S1463423625000222","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Aim: This study aims to assess the effect of primary health care (PHC) service provision continuity on inpatient admissions for people with chronic diseases in Estonia.
Background: Non-communicable diseases (NCDs) were collectively responsible for more than 7 out of 10 deaths worldwide in 2019. As the burden of NCDs increases, PHC has an increased role of coordinating care management. High-performing PHC can reduce unnecessary hospitalizations. Estonia has a strong PHC system focusing on multidisciplinary care. Yet it has not been evaluated for its effect on hospitalizations. Therefore, it is imperative to evaluate PHC continuity to improve care for NCD patients.
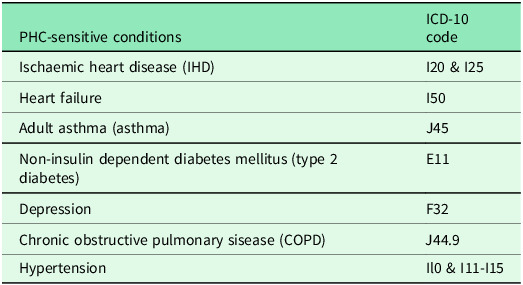
Methods: This study used routinely collected electronic medical billing data of the Estonian population aged 15 years or older from 2005 to 2020 identifying patients with seven ambulatory care sensitive chronic (ACSC) conditions. We developed an indicator to describe the continuity of PHC. Charlson Comorbidity Index (CCI) was used to assess the impact of comorbidities and we controlled the patient's age, gender, county of residency and socio-economic status. We estimated multilevel logistic regression models with family doctor patient list random effects to assess how the odds of hospitalization depend on continuity of care, allowing for confounders.
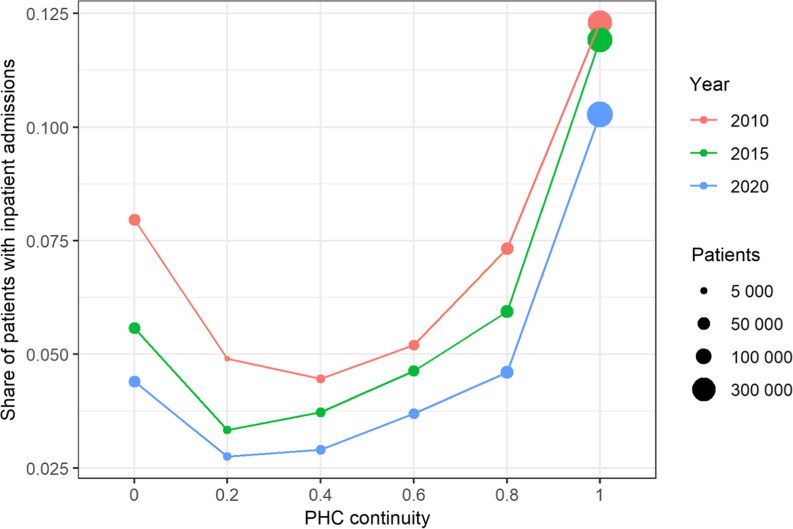
Findings: We identified that 45% of the adult Estonian population had at least one of the target diagnoses. Among the target population, 96% had contact with their PHC providers. We found that there is a non-linear relationship between PHC continuity and patient outcomes. Any contact with PHC provider during the past 5 years decreases odds for hospitalization, but hospitalization risk is higher for people who are elderly and have higher CCI score. We found that after accounting for patient characteristics, differences among patient lists minimally impact outcomes. Further research should explore policies to better support family doctors in reducing hospitalizations for chronic patients.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


