Marilia B Voigt, Patrick A Kupczyk, Alexander Kania, Carsten Meyer, Julia Wagenpfeil, Tatjana Dell, Claus-Christian Pieper, Julian A Luetkens, Daniel Kuetting
{"title":"Interventional treatment of peripancreatic aneurysms: can one strategy fit all?","authors":"Marilia B Voigt, Patrick A Kupczyk, Alexander Kania, Carsten Meyer, Julia Wagenpfeil, Tatjana Dell, Claus-Christian Pieper, Julian A Luetkens, Daniel Kuetting","doi":"10.1186/s42155-025-00533-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To identify the frequency and association of visceral arterial (VA) stenosis in peripancreatic aneurysms (PPAs) and to develop a uniform, more detailed treatment strategy for PPAs in case of accompanying VA stenosis, as current guidelines do not adequately address this constellation.</p><p><strong>Materials and methods: </strong>Patients with PPAs diagnosed at a tertiary care hospital were retrospectively analyzed. In case of multiple PPAs, the aneurysm with the highest aneurysm-to-vessel ratio (AVR) within the celiac-mesenteric collateral circulation was classified as the primary aneurysm and categorized as \"critical\" or \"non-critical\" based on the risk of organ ischemia. Celiac artery and superior mesenteric artery stenoses were graded as low (< 50%), high (> 50%), or total occlusion. Treatment strategies were based on VA stenosis severity, aneurysm classification, and morphology. Treatment strategies included endovascular, surgical and watch-and-wait management.</p><p><strong>Results: </strong>Thirty-one patients with PPAs were included with a total of 53 aneurysms; mean aneurysm size: 12.5 ± 7.9 mm (range 5-38 mm), AVR: 3.5 ± 2.1 (range 1-11.3). The superior and inferior pancreaticoduodenal arteries as well as the pancreaticoduodenal arcade were affected in most cases (67.9%). AVR was significantly higher in cases of aneurysm rupture (6.2 ± 2.8; p = 0.031). Celiac artery stenosis was present in 87.1%. Aneurysm size and occurrence of active bleeding did not correlate (p = 0.925). 11 patients presented with critical aneurysms, with 10 patients requiring individually tailored treatment. Non-critical aneurysms were treated with coil embolization in most cases.</p><p><strong>Conclusion: </strong>CA stenosis, aneurysm position, and AVR significantly influence treatment decisions. Individualized approaches based on anatomical and hemodynamic factors are needed in PPA treatment.</p>","PeriodicalId":52351,"journal":{"name":"CVIR Endovascular","volume":"8 1","pages":"23"},"PeriodicalIF":1.5000,"publicationDate":"2025-03-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11923352/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CVIR Endovascular","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s42155-025-00533-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: To identify the frequency and association of visceral arterial (VA) stenosis in peripancreatic aneurysms (PPAs) and to develop a uniform, more detailed treatment strategy for PPAs in case of accompanying VA stenosis, as current guidelines do not adequately address this constellation.
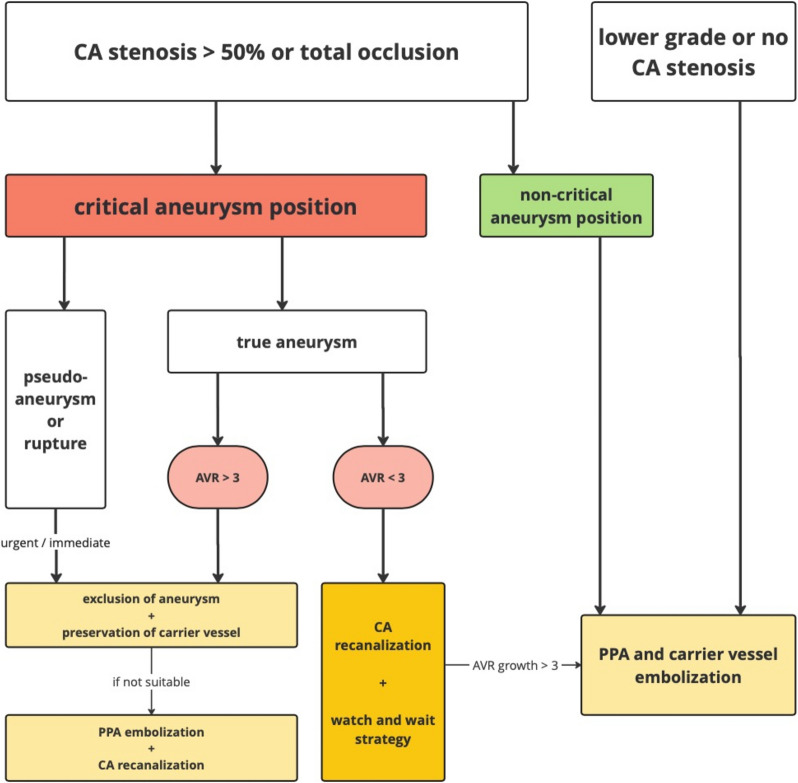
Materials and methods: Patients with PPAs diagnosed at a tertiary care hospital were retrospectively analyzed. In case of multiple PPAs, the aneurysm with the highest aneurysm-to-vessel ratio (AVR) within the celiac-mesenteric collateral circulation was classified as the primary aneurysm and categorized as "critical" or "non-critical" based on the risk of organ ischemia. Celiac artery and superior mesenteric artery stenoses were graded as low (< 50%), high (> 50%), or total occlusion. Treatment strategies were based on VA stenosis severity, aneurysm classification, and morphology. Treatment strategies included endovascular, surgical and watch-and-wait management.
Results: Thirty-one patients with PPAs were included with a total of 53 aneurysms; mean aneurysm size: 12.5 ± 7.9 mm (range 5-38 mm), AVR: 3.5 ± 2.1 (range 1-11.3). The superior and inferior pancreaticoduodenal arteries as well as the pancreaticoduodenal arcade were affected in most cases (67.9%). AVR was significantly higher in cases of aneurysm rupture (6.2 ± 2.8; p = 0.031). Celiac artery stenosis was present in 87.1%. Aneurysm size and occurrence of active bleeding did not correlate (p = 0.925). 11 patients presented with critical aneurysms, with 10 patients requiring individually tailored treatment. Non-critical aneurysms were treated with coil embolization in most cases.
Conclusion: CA stenosis, aneurysm position, and AVR significantly influence treatment decisions. Individualized approaches based on anatomical and hemodynamic factors are needed in PPA treatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


