Antonia Bosworth Smith, Ubong Silas, Alex Veloz, Peter Mallow, Barbara Pisani, Diana Bonderman, Rhodri Saunders
{"title":"Cost-Effectiveness Analysis of a Heart Failure Management System in the United States.","authors":"Antonia Bosworth Smith, Ubong Silas, Alex Veloz, Peter Mallow, Barbara Pisani, Diana Bonderman, Rhodri Saunders","doi":"10.36469/001c.130066","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> The disease burden of heart failure is mainly driven by high hospital readmission rates. Remote monitoring devices can be used to assess the status of patients after discharge and identify early signs of worsening symptoms. Initial studies indicated that Heart Failure Management System (HFMS), a novel monitoring device, can prevent hospital readmission. <b>Objective:</b> To determine the cost effectiveness of HFMS compared with standard of care (SOC) in the United States. <b>Methods:</b> A Markov model was developed to follow patients after their discharge from index hospitalization for heart failure. The costs and outcomes were estimated for 5 years. The patient cohort was initially in \"outpatient care,\" where they are at risk of an emergency room visit or hospital readmission. If hospitalized, patients returned to a second outpatient care health state. An \"escalation of care\" (eg, surgical intervention) may have removed patients from the intervention. The model took the payer perspective with costs in 2022 US dollars. The incremental cost-effectiveness ratio measured effectiveness through hospital readmissions. The willingness-to-pay threshold was set to the published cost of a heart failure rehospitalization ($10 737). Sensitivity and scenario analyses explored the robustness of the model to changes in inputs. <b>Results:</b> Compared with SOC, HFMS reduced the mean cost of care by <math><mn>6723</mn> <mo>(</mo></math> 155 122 vs $161 846) over the 5-year period. The mean number of hospital readmissions was reduced to 1.075 with HFMS from 1.201 with SOC (-0.126 events). The incremental cost-effectiveness ratio showed that HFMS was a dominant strategy compared with SOC, leading to reduced costs and hospital readmissions in 93.4% of the 1000 Monte Carlo simulations; 94.1% of the simulations fell below the willingness-topay threshold. Savings with HFMS emerged from the third month. <b>Discussion:</b> The results indicated the cost-effectiveness of HFMS compared with SOC. The sensitivity analyses supported this finding. Reducing costly hospital readmissions may help to alleviate the burden of heart failure. Longer-term data on HFMS are encouraged to confirm or contest the model outcomes. <b>Conclusions:</b> The use of HFMS is expected to save costs and reduce hospitalizations over a 5-year period compared with the current SOC.</p>","PeriodicalId":16012,"journal":{"name":"Journal of Health Economics and Outcomes Research","volume":"12 1","pages":"113-119"},"PeriodicalIF":2.3000,"publicationDate":"2025-03-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11922182/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Health Economics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36469/001c.130066","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
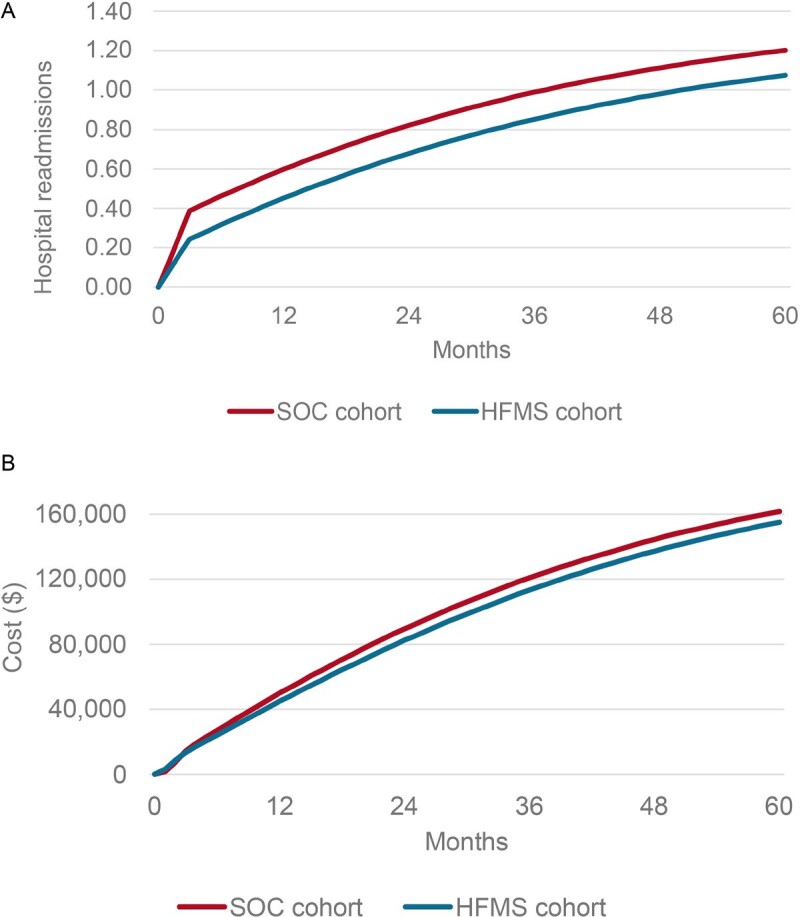
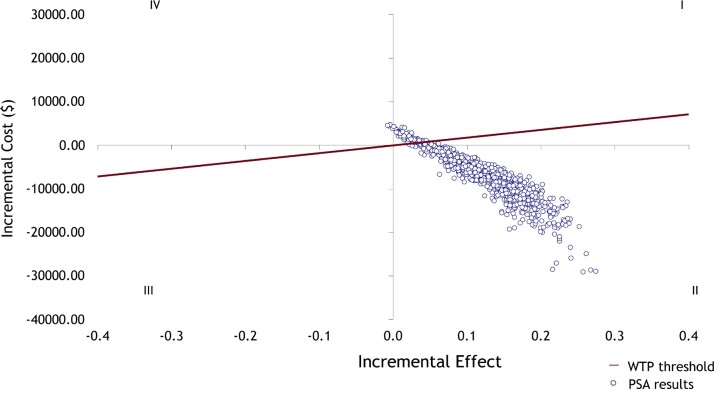
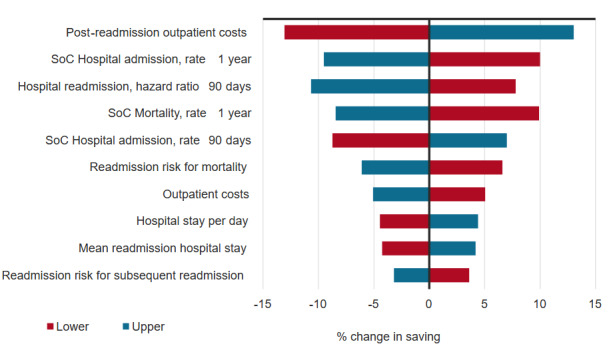
Background: The disease burden of heart failure is mainly driven by high hospital readmission rates. Remote monitoring devices can be used to assess the status of patients after discharge and identify early signs of worsening symptoms. Initial studies indicated that Heart Failure Management System (HFMS), a novel monitoring device, can prevent hospital readmission. Objective: To determine the cost effectiveness of HFMS compared with standard of care (SOC) in the United States. Methods: A Markov model was developed to follow patients after their discharge from index hospitalization for heart failure. The costs and outcomes were estimated for 5 years. The patient cohort was initially in "outpatient care," where they are at risk of an emergency room visit or hospital readmission. If hospitalized, patients returned to a second outpatient care health state. An "escalation of care" (eg, surgical intervention) may have removed patients from the intervention. The model took the payer perspective with costs in 2022 US dollars. The incremental cost-effectiveness ratio measured effectiveness through hospital readmissions. The willingness-to-pay threshold was set to the published cost of a heart failure rehospitalization ($10 737). Sensitivity and scenario analyses explored the robustness of the model to changes in inputs. Results: Compared with SOC, HFMS reduced the mean cost of care by 155 122 vs $161 846) over the 5-year period. The mean number of hospital readmissions was reduced to 1.075 with HFMS from 1.201 with SOC (-0.126 events). The incremental cost-effectiveness ratio showed that HFMS was a dominant strategy compared with SOC, leading to reduced costs and hospital readmissions in 93.4% of the 1000 Monte Carlo simulations; 94.1% of the simulations fell below the willingness-topay threshold. Savings with HFMS emerged from the third month. Discussion: The results indicated the cost-effectiveness of HFMS compared with SOC. The sensitivity analyses supported this finding. Reducing costly hospital readmissions may help to alleviate the burden of heart failure. Longer-term data on HFMS are encouraged to confirm or contest the model outcomes. Conclusions: The use of HFMS is expected to save costs and reduce hospitalizations over a 5-year period compared with the current SOC.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


