Dimitrios Starvridis, Arian Arjomandi Rad, Paola Keese Montanhesi, Hristo Kirov, Max Wacker, Panagiotis Tasoudis, Murat Mukharyamov, Ricardo E Treml, Jens Wippermann, Torsten Doenst, Ibrahim Sultan, Michel Pompeu Sá, Tulio Caldonazo
{"title":"Mini-Sternotomy vs. Right Anterior Mini-Thoracotomy for Surgical Aortic Valve Replacement - A Systematic Review and Meta-Analysis.","authors":"Dimitrios Starvridis, Arian Arjomandi Rad, Paola Keese Montanhesi, Hristo Kirov, Max Wacker, Panagiotis Tasoudis, Murat Mukharyamov, Ricardo E Treml, Jens Wippermann, Torsten Doenst, Ibrahim Sultan, Michel Pompeu Sá, Tulio Caldonazo","doi":"10.21470/1678-9741-2024-0211","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Minimally invasive techniques for aortic valve replacement have become increasingly popular. The most common minimally invasive approaches are mini-sternotomy and right anterior mini-thoracotomy. We aimed to review the literature and compare clinical outcomes for these two approaches.</p><p><strong>Methods: </strong>Three databases were assessed. The primary endpoint was perioperative mortality. The secondary endpoints were reoperation for bleeding, stroke, operation duration, intensive care unit length of stay, cardiopulmonary bypass time, cross-clamping time, hospital length of stay, paravalvular leak, renal complications, conversion to full sternotomy, permanent pacemaker implantation, and wound infection. Random effects models were performed.</p><p><strong>Results: </strong>Ten studies were included in the meta-analysis (30,524 patients). There was no difference in perioperative mortality between groups (odds ratio: 0.83; 95% confidence interval 0.57-1.21; P=0.33). In comparison with mini-sternotomy, right anterior mini-thoracotomy showed higher rates of reoperation for bleeding (odds ratio: 0.69; 95% confidence interval 0.50-0.97; P=0.03), lower rates of stroke (odds ratio: 1.27; 95% confidence interval 1.01-1.60; P=0.04), and longer operation duration (standard mean difference: -0.58; 95% confidence interval -1.01 to -0.14; P=0.01). Other secondary endpoints were not statistically significant.</p><p><strong>Conclusion: </strong>The results suggest that both techniques present similar perioperative mortality rates for aortic valve replacement. However, right anterior mini-thoracotomy is associated with higher rates of reoperation for bleeding, lower rates of stroke, and longer operation duration time.</p>","PeriodicalId":72457,"journal":{"name":"Brazilian journal of cardiovascular surgery","volume":"40 3","pages":"e20240211"},"PeriodicalIF":1.2000,"publicationDate":"2025-03-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11925351/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brazilian journal of cardiovascular surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21470/1678-9741-2024-0211","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Minimally invasive techniques for aortic valve replacement have become increasingly popular. The most common minimally invasive approaches are mini-sternotomy and right anterior mini-thoracotomy. We aimed to review the literature and compare clinical outcomes for these two approaches.
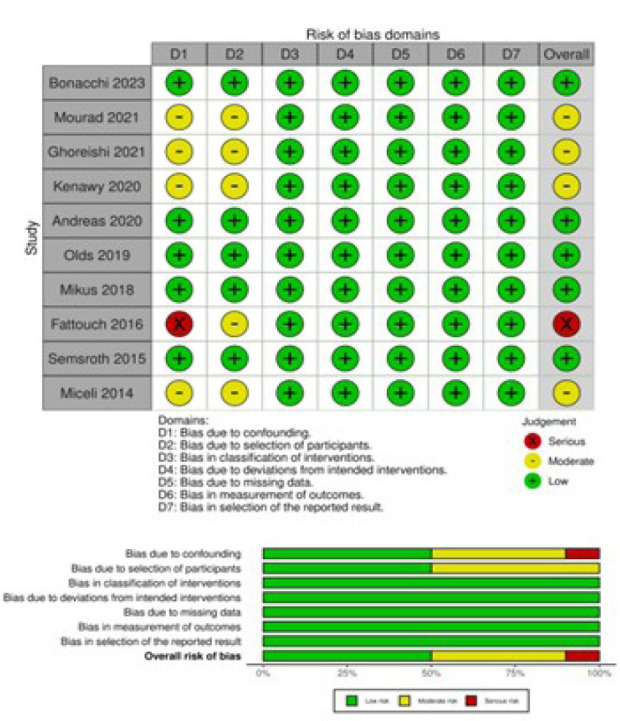
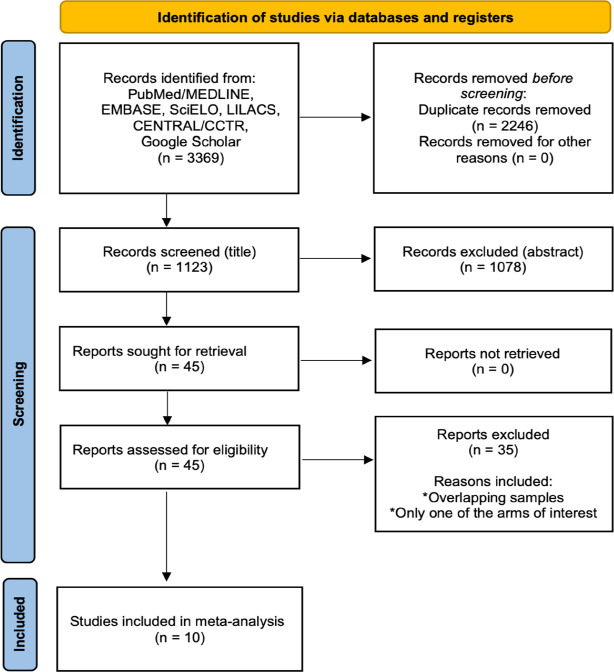
Methods: Three databases were assessed. The primary endpoint was perioperative mortality. The secondary endpoints were reoperation for bleeding, stroke, operation duration, intensive care unit length of stay, cardiopulmonary bypass time, cross-clamping time, hospital length of stay, paravalvular leak, renal complications, conversion to full sternotomy, permanent pacemaker implantation, and wound infection. Random effects models were performed.
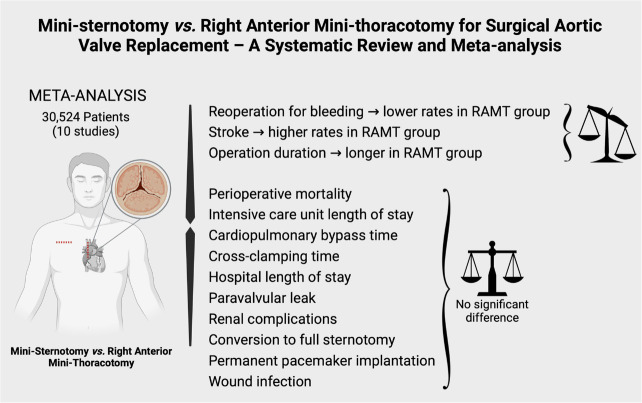
Results: Ten studies were included in the meta-analysis (30,524 patients). There was no difference in perioperative mortality between groups (odds ratio: 0.83; 95% confidence interval 0.57-1.21; P=0.33). In comparison with mini-sternotomy, right anterior mini-thoracotomy showed higher rates of reoperation for bleeding (odds ratio: 0.69; 95% confidence interval 0.50-0.97; P=0.03), lower rates of stroke (odds ratio: 1.27; 95% confidence interval 1.01-1.60; P=0.04), and longer operation duration (standard mean difference: -0.58; 95% confidence interval -1.01 to -0.14; P=0.01). Other secondary endpoints were not statistically significant.
Conclusion: The results suggest that both techniques present similar perioperative mortality rates for aortic valve replacement. However, right anterior mini-thoracotomy is associated with higher rates of reoperation for bleeding, lower rates of stroke, and longer operation duration time.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


