Andreas Koköfer, Christian Dinges, Crispiana Cozowicz, Bernhard Wernly, Niklas Rodemund
{"title":"Nocturnal elective coronary artery bypass grafting (CABG) surgery is not associated with increased one-year mortality.","authors":"Andreas Koköfer, Christian Dinges, Crispiana Cozowicz, Bernhard Wernly, Niklas Rodemund","doi":"10.1186/s13037-025-00430-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Elective coronary artery bypass grafting (CABG) surgeries are increasingly scheduled during nighttime or after-hours. This poses unique challenges, such as reduced staffing, disrupted circadian rhythms, and increased fatigue, which may potentially affect outcomes. Despite growing evidence on the impact of daytime on cardiac surgery outcome, results remain inconclusive. The current study aims to investigate a potential association between surgery timing (daytime: 7:00 AM to 7:00 PM vs. nighttime: 7:00 PM to 7:00 AM) and long-term survival in patients undergoing elective CABG.</p><p><strong>Methods: </strong>In this retrospective single-institution cohort study at the University Clinic Salzburg, Austria, we analyzed elective CABG surgeries performed between January 1, 2017, and December 31, 2021. The primary hypothesis was that nighttime elective CABG surgeries have worse long-term survival. Among 2,179 cardiac surgical procedures, 723 elective CABG surgeries were identified and analyzed. Long-term survival was assessed using Cox proportional hazard modeling, while secondary outcomes, including 30-day and one-year mortality rates, were evaluated through multiple linear regression analysis.</p><p><strong>Results: </strong>The one-year mortality rate was 2.6% (n = 19) for the observation period. Of the 723 patients, 646 (89.35%) underwent daytime surgery, and 77 (10.65%) had nighttime surgery. The median EuroScore II was 1.50 [1.00, 2.60] for daytime surgeries and 1.70 [1.10, 3.10] for nighttime surgeries (p = 0.111). There was no association between nighttime surgery and long-term mortality (aHR: 1.624, 95% CI: 0.589 to 3.662, p = 0.3179). Multivariable logistic regression analysis confirmed that nighttime surgeries were not significantly associated with increased one-year mortality (aOR: 1.089, 95% CI: 0.208 to 3.711, p = 0.905). No deaths occurred within 30 days in either group.</p><p><strong>Conclusion: </strong>This analysis found no significant association between nocturnal elective CABG operations and increased long-term or one-year mortality. This study did not aim to evaluate the economics of nocturnal surgeries at the investigated institution. To confirm our results that there is no increased morbidity and mortality associated with nocturnal CABG operations, and to understand the economic impact of nocturnal surgeries, prospective randomized studies would be necessary.</p>","PeriodicalId":46782,"journal":{"name":"Patient Safety in Surgery","volume":"19 1","pages":"8"},"PeriodicalIF":2.1000,"publicationDate":"2025-03-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11912614/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Patient Safety in Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13037-025-00430-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Elective coronary artery bypass grafting (CABG) surgeries are increasingly scheduled during nighttime or after-hours. This poses unique challenges, such as reduced staffing, disrupted circadian rhythms, and increased fatigue, which may potentially affect outcomes. Despite growing evidence on the impact of daytime on cardiac surgery outcome, results remain inconclusive. The current study aims to investigate a potential association between surgery timing (daytime: 7:00 AM to 7:00 PM vs. nighttime: 7:00 PM to 7:00 AM) and long-term survival in patients undergoing elective CABG.
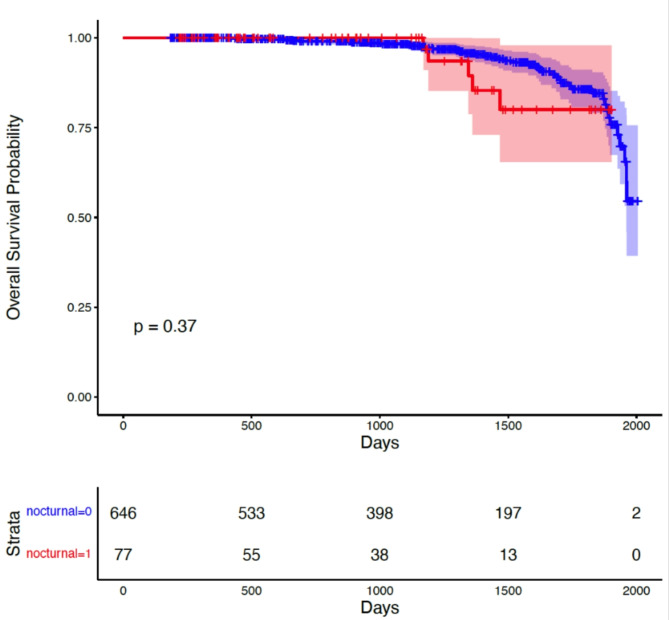
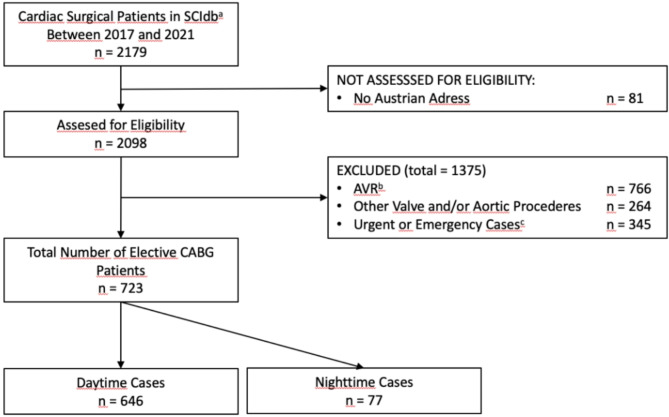
Methods: In this retrospective single-institution cohort study at the University Clinic Salzburg, Austria, we analyzed elective CABG surgeries performed between January 1, 2017, and December 31, 2021. The primary hypothesis was that nighttime elective CABG surgeries have worse long-term survival. Among 2,179 cardiac surgical procedures, 723 elective CABG surgeries were identified and analyzed. Long-term survival was assessed using Cox proportional hazard modeling, while secondary outcomes, including 30-day and one-year mortality rates, were evaluated through multiple linear regression analysis.
Results: The one-year mortality rate was 2.6% (n = 19) for the observation period. Of the 723 patients, 646 (89.35%) underwent daytime surgery, and 77 (10.65%) had nighttime surgery. The median EuroScore II was 1.50 [1.00, 2.60] for daytime surgeries and 1.70 [1.10, 3.10] for nighttime surgeries (p = 0.111). There was no association between nighttime surgery and long-term mortality (aHR: 1.624, 95% CI: 0.589 to 3.662, p = 0.3179). Multivariable logistic regression analysis confirmed that nighttime surgeries were not significantly associated with increased one-year mortality (aOR: 1.089, 95% CI: 0.208 to 3.711, p = 0.905). No deaths occurred within 30 days in either group.
Conclusion: This analysis found no significant association between nocturnal elective CABG operations and increased long-term or one-year mortality. This study did not aim to evaluate the economics of nocturnal surgeries at the investigated institution. To confirm our results that there is no increased morbidity and mortality associated with nocturnal CABG operations, and to understand the economic impact of nocturnal surgeries, prospective randomized studies would be necessary.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


