Mohamed Fehmi Bayar, Emna Bennour, Zied Ibn El Hadj, Oumayma Zidi, Afef Ben Hlima, Ikram Kammoun
{"title":"Sudden cardiac death in hyperthrophic cardiomyopathy: Comparison of predictive models.","authors":"Mohamed Fehmi Bayar, Emna Bennour, Zied Ibn El Hadj, Oumayma Zidi, Afef Ben Hlima, Ikram Kammoun","doi":"10.62438/tunismed.v103i2.4779","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Sudden cardiac death (SCD) risk stratification for primary prevention in patients with sarcomeric hypertrophic cardiomyopathy (HCM) has recently been reinforced by the establishment of a new model by the American College of Cardiology (ACC). This algorithm was characterized by a different approach compared to the previous HCM Risk Score.</p><p><strong>Aim: </strong>The objective of this study was to compare risk stratification using both the European society of cardiology (ESC) and the ACC risk scores.</p><p><strong>Methods: </strong>This was an observational, cohort-type prognostic study with retrospective data collection. Patients were classified according to their rhythmic risk estimated by both models and followed for a period of at least one year.</p><p><strong>Results: </strong>Forty-seven patients were followed over a mean period of 32,4 months. The mean age of our patients was 55 years ± 14 years. We found a weak concordance between the two models (Kappa = 0.28). Four patients (9 %) presented arrhythmogenic events. The ACC algorithm indicated the implantation of an implantable cardioverter defibrillator (ICD) for these four patients whereas the HCM Risk Score indicated only two. The American algorithm had a better predictive potency with an area under the ROC curve of 0.785 compared to 0.654 with the HCM Risk Score with an NRI of 0.35. However, the number of ICDs to be implanted according to this algorithm was increased by 1.6 times.</p><p><strong>Conclusion: </strong>The ACC algorithm was more efficient in detecting high-risk patients, but it considerably increased the number of ICDs indicated.</p>","PeriodicalId":38818,"journal":{"name":"Tunisie Medicale","volume":"103 2","pages":"264-269"},"PeriodicalIF":0.0000,"publicationDate":"2025-02-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12034364/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Tunisie Medicale","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.62438/tunismed.v103i2.4779","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Sudden cardiac death (SCD) risk stratification for primary prevention in patients with sarcomeric hypertrophic cardiomyopathy (HCM) has recently been reinforced by the establishment of a new model by the American College of Cardiology (ACC). This algorithm was characterized by a different approach compared to the previous HCM Risk Score.
Aim: The objective of this study was to compare risk stratification using both the European society of cardiology (ESC) and the ACC risk scores.
Methods: This was an observational, cohort-type prognostic study with retrospective data collection. Patients were classified according to their rhythmic risk estimated by both models and followed for a period of at least one year.
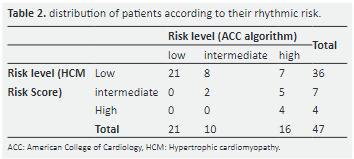
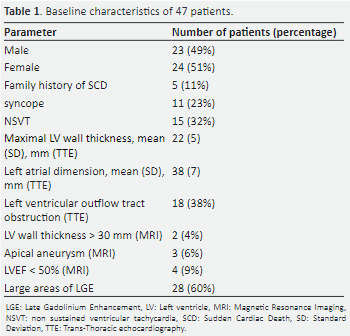
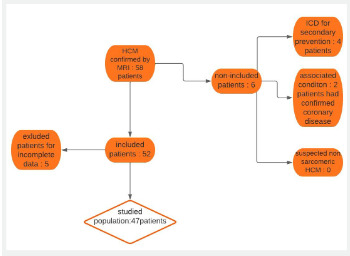
Results: Forty-seven patients were followed over a mean period of 32,4 months. The mean age of our patients was 55 years ± 14 years. We found a weak concordance between the two models (Kappa = 0.28). Four patients (9 %) presented arrhythmogenic events. The ACC algorithm indicated the implantation of an implantable cardioverter defibrillator (ICD) for these four patients whereas the HCM Risk Score indicated only two. The American algorithm had a better predictive potency with an area under the ROC curve of 0.785 compared to 0.654 with the HCM Risk Score with an NRI of 0.35. However, the number of ICDs to be implanted according to this algorithm was increased by 1.6 times.
Conclusion: The ACC algorithm was more efficient in detecting high-risk patients, but it considerably increased the number of ICDs indicated.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


