Brachial plexus block versus local anesthesia for percutaneous transluminal angioplasty of dysfunctional arteriovenous fistula: 12-month results of a propensity score weighted study.
Xiaojing Wang, Yuli Wang, Yiping Zhao, Yinan Li, Xiangjiang Guo, Lan Zhang, Jiaquan Chen, Qihong Ni
{"title":"Brachial plexus block versus local anesthesia for percutaneous transluminal angioplasty of dysfunctional arteriovenous fistula: 12-month results of a propensity score weighted study.","authors":"Xiaojing Wang, Yuli Wang, Yiping Zhao, Yinan Li, Xiangjiang Guo, Lan Zhang, Jiaquan Chen, Qihong Ni","doi":"10.1080/0886022X.2025.2477834","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The study aimed to compare ultrasound-guided brachial plexus block (BPB) with local anesthesia (LA) on efficacy, safety and 12-month patency rate for percutaneous transluminal angioplasty (PTA) treatment of dysfunctional arteriovenous fistula (AVF).</p><p><strong>Methods: </strong>Consecutive patients with dysfunctional AVF who underwent PTA from January 2021 to December 2022 were included. Overlap weighting was performed to adjust for significant differences between the two groups. The primary efficacy outcomes included visual analogue scale (VAS) score and 12-month target-lesion primary patency rate. The secondary efficacy outcomes included target-lesion primary-assisted patency rate, secondary patency rate, access-circuit thrombosis rate, access-circuit reintervention rate, and number of reinterventions within 12 months. Univariate analysis and multivariate analysis by log-binomial regression were used to identify the independent factors associated with intraoperative pain.</p><p><strong>Results: </strong>218 patients were included in the study: 82 patients underwent PTA under BPB and 136 patients underwent PTA under LA. After overlap weighting, the baseline, lesion characteristics and intraoperative details had no significant difference between the two groups. Patients under BPB had significantly lower VAS scores than those under LA (2.4 ± 1.4 vs 5.1 ± 1.9, <i>p</i> < 0.001). The 12-month target-lesion primary patency rate was significantly higher in the BPB group than that in the LA group (58.3% vs 40.0%, <i>p</i> = 0.037). The 12-month target-lesion primary-assisted patency rate and access-circuit secondary patency rate were significantly higher in the BPB group than those in the LA group (<i>p</i> = 0.023 and <i>p</i> = 0.028). The access-circuit thrombosis rate was significantly lower in the BPB group (10.0%) than that in the LA group (28.3%) (<i>p</i> = 0.011). BPB was the only independent factor associated with mild pain (<i>p</i> < 0.001, OR: 0.037, 95%CI: 0.011-0.119).</p><p><strong>Conclusions: </strong>BPB could decrease the intraoperative pain and improve the 12-month primary patency rates compared with LA for patients underwent PTA treatment of dysfunctional AVF.</p>","PeriodicalId":20839,"journal":{"name":"Renal Failure","volume":"47 1","pages":"2477834"},"PeriodicalIF":3.0000,"publicationDate":"2025-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11915726/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Renal Failure","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1080/0886022X.2025.2477834","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/17 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: The study aimed to compare ultrasound-guided brachial plexus block (BPB) with local anesthesia (LA) on efficacy, safety and 12-month patency rate for percutaneous transluminal angioplasty (PTA) treatment of dysfunctional arteriovenous fistula (AVF).
Methods: Consecutive patients with dysfunctional AVF who underwent PTA from January 2021 to December 2022 were included. Overlap weighting was performed to adjust for significant differences between the two groups. The primary efficacy outcomes included visual analogue scale (VAS) score and 12-month target-lesion primary patency rate. The secondary efficacy outcomes included target-lesion primary-assisted patency rate, secondary patency rate, access-circuit thrombosis rate, access-circuit reintervention rate, and number of reinterventions within 12 months. Univariate analysis and multivariate analysis by log-binomial regression were used to identify the independent factors associated with intraoperative pain.
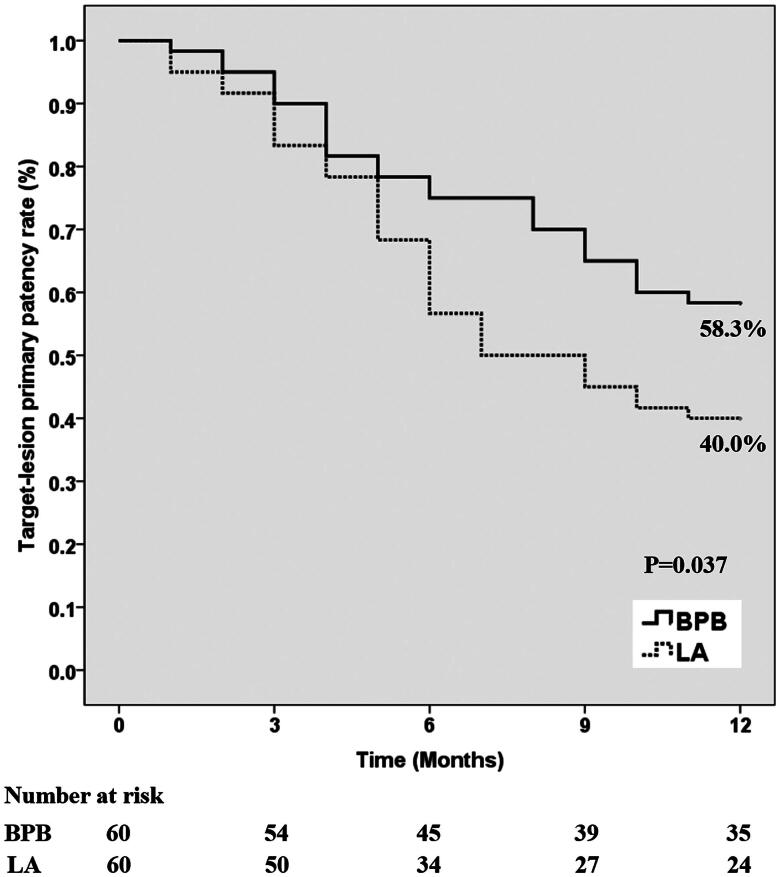
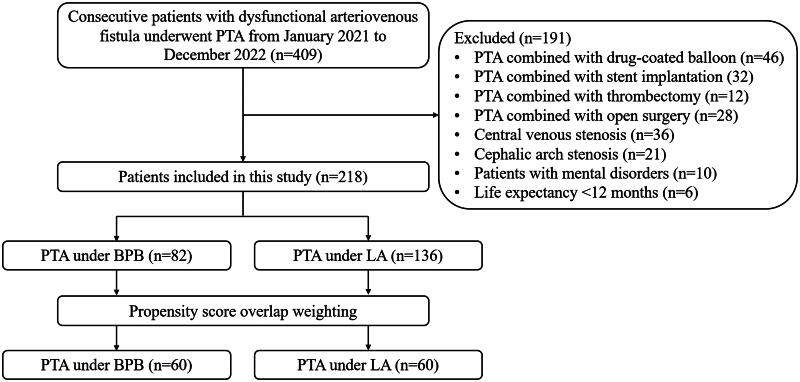
Results: 218 patients were included in the study: 82 patients underwent PTA under BPB and 136 patients underwent PTA under LA. After overlap weighting, the baseline, lesion characteristics and intraoperative details had no significant difference between the two groups. Patients under BPB had significantly lower VAS scores than those under LA (2.4 ± 1.4 vs 5.1 ± 1.9, p < 0.001). The 12-month target-lesion primary patency rate was significantly higher in the BPB group than that in the LA group (58.3% vs 40.0%, p = 0.037). The 12-month target-lesion primary-assisted patency rate and access-circuit secondary patency rate were significantly higher in the BPB group than those in the LA group (p = 0.023 and p = 0.028). The access-circuit thrombosis rate was significantly lower in the BPB group (10.0%) than that in the LA group (28.3%) (p = 0.011). BPB was the only independent factor associated with mild pain (p < 0.001, OR: 0.037, 95%CI: 0.011-0.119).
Conclusions: BPB could decrease the intraoperative pain and improve the 12-month primary patency rates compared with LA for patients underwent PTA treatment of dysfunctional AVF.
期刊介绍:
Renal Failure primarily concentrates on acute renal injury and its consequence, but also addresses advances in the fields of chronic renal failure, hypertension, and renal transplantation. Bringing together both clinical and experimental aspects of renal failure, this publication presents timely, practical information on pathology and pathophysiology of acute renal failure; nephrotoxicity of drugs and other substances; prevention, treatment, and therapy of renal failure; renal failure in association with transplantation, hypertension, and diabetes mellitus.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


