Constrictive Pericarditis in a Hemodialysis Patient Who Presented with Rapidly Progressive Pericardial Calcification: A Diagnostic Challenge - A Case Report.
{"title":"Constrictive Pericarditis in a Hemodialysis Patient Who Presented with Rapidly Progressive Pericardial Calcification: A Diagnostic Challenge - A Case Report.","authors":"Oho Tsunematsu, Shin-Ichi Takeda, Mitsutaka Yamaguchi, Miwa Kaneko, Kazuho Oe, Yoshiaki Murakami, Daisuke Nagata","doi":"10.1159/000543999","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Constrictive pericarditis (CP) is characterized by impaired diastolic filling of the ventricles, which typically causes right heart failure. Its diagnosis may be challenging because it mimics other disorders. Furthermore, prompt diagnosis and treatment are more crucial in cases of hemodialysis; otherwise, maintenance dialysis would be hampered by severe hypotension.</p><p><strong>Case presentation: </strong>We report the case of a 53-year-old man on hemodialysis who developed CP with shock. His blood pressure was 55/30 mm Hg at the time of hospitalization due to presyncope. He continued hemodialysis but with some difficulty. However, right pleural effusion persisted because of impaired fluid removal by hemodialysis. Despite such severe manifestations, the distinctive clinical features of CP were lacking. By carefully evaluating the time course of computed tomography images, progressive calcification in the pericardium emerged as a significant clue. Cardiac catheterization subsequently revealed a dip-and-plateau pattern of right ventricular pressure, which led to a definitive diagnosis of CP. Soon after the diagnosis, he underwent successful surgery.</p><p><strong>Conclusion: </strong>An important finding was that, unlike calcific lesions in the general dialysis population, the patient's calcific lesions were mostly confined to the pericardium and progressed on a monthly basis. Thus, the present case may provide deep insight into the diagnosis of CP and the management of hemodialysis patients with severe hypotension.</p>","PeriodicalId":9599,"journal":{"name":"Case Reports in Nephrology and Dialysis","volume":"15 1","pages":"33-40"},"PeriodicalIF":0.9000,"publicationDate":"2025-02-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11908808/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Nephrology and Dialysis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000543999","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Constrictive pericarditis (CP) is characterized by impaired diastolic filling of the ventricles, which typically causes right heart failure. Its diagnosis may be challenging because it mimics other disorders. Furthermore, prompt diagnosis and treatment are more crucial in cases of hemodialysis; otherwise, maintenance dialysis would be hampered by severe hypotension.
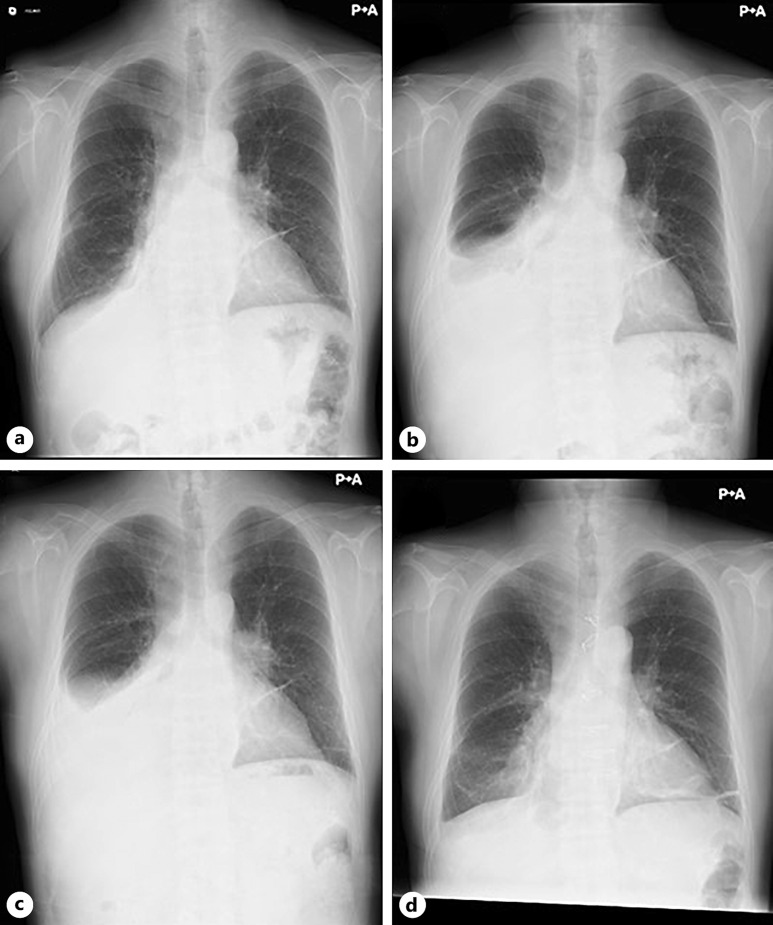
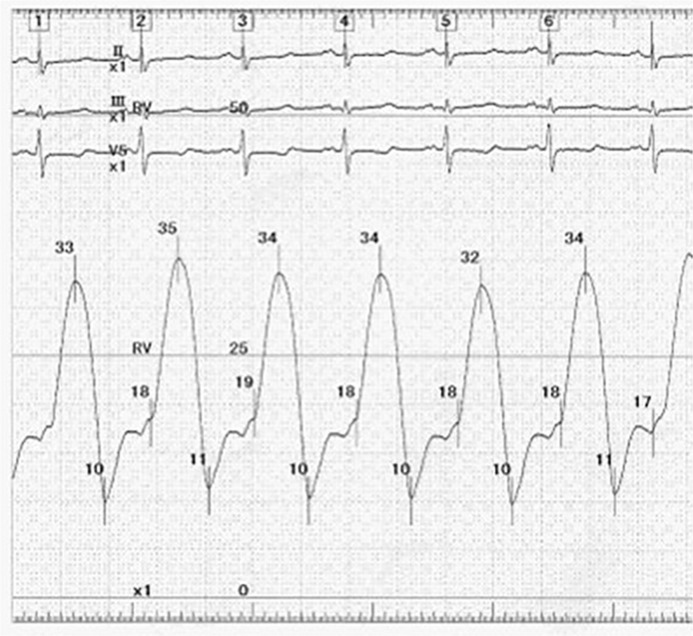
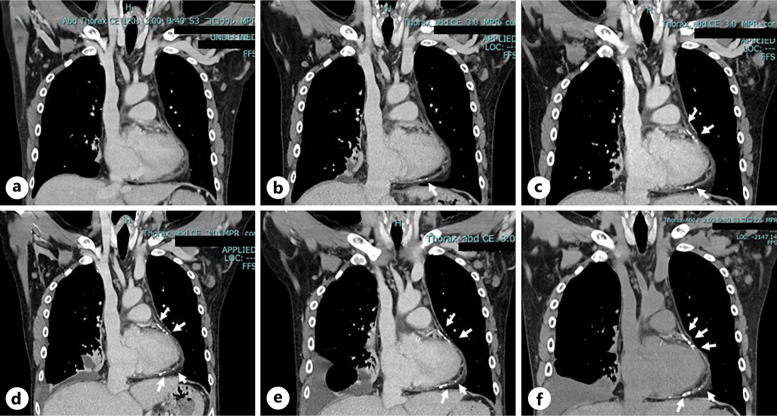
Case presentation: We report the case of a 53-year-old man on hemodialysis who developed CP with shock. His blood pressure was 55/30 mm Hg at the time of hospitalization due to presyncope. He continued hemodialysis but with some difficulty. However, right pleural effusion persisted because of impaired fluid removal by hemodialysis. Despite such severe manifestations, the distinctive clinical features of CP were lacking. By carefully evaluating the time course of computed tomography images, progressive calcification in the pericardium emerged as a significant clue. Cardiac catheterization subsequently revealed a dip-and-plateau pattern of right ventricular pressure, which led to a definitive diagnosis of CP. Soon after the diagnosis, he underwent successful surgery.
Conclusion: An important finding was that, unlike calcific lesions in the general dialysis population, the patient's calcific lesions were mostly confined to the pericardium and progressed on a monthly basis. Thus, the present case may provide deep insight into the diagnosis of CP and the management of hemodialysis patients with severe hypotension.
简介:缩窄性心包炎(CP)的特征是心室舒张充盈受损,通常导致右心衰。它的诊断可能具有挑战性,因为它与其他疾病相似。此外,在血液透析病例中,及时诊断和治疗更为重要;否则,维持性透析将因严重低血压而受阻。病例介绍:我们报告一例53岁的男性血液透析谁发展CP与休克。因晕厥前期入院时血压为55/30 mm Hg。他继续进行血液透析,但有些困难。然而,由于血液透析的液体清除受损,右侧胸腔积液持续存在。尽管有如此严重的表现,但CP缺乏鲜明的临床特征。通过仔细评估计算机断层图像的时间过程,心包的进行性钙化成为一个重要的线索。随后的心导管检查显示右心室压力呈下降和平台型,最终诊断为CP。诊断后不久,他接受了成功的手术。结论:一个重要的发现是,与普通透析人群中的钙化病变不同,患者的钙化病变主要局限于心包,并以每月为基础进展。因此,本病例可能为CP的诊断和严重低血压血液透析患者的处理提供深入的见解。
期刊介绍:
This peer-reviewed online-only journal publishes original case reports covering the entire spectrum of nephrology and dialysis, including genetic susceptibility, clinical presentation, diagnosis, treatment or prevention, toxicities of therapy, critical care, supportive care, quality-of-life and survival issues. The journal will also accept case reports dealing with the use of novel technologies, both in the arena of diagnosis and treatment. Supplementary material is welcomed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


