{"title":"Adnexal Incarceration in a Posterior Pelvic Peritoneal Defect Associated with Ovarian Torsion: A Case Report.","authors":"Lina Qattea, Wafa Alshahrani, Samaher Samer Alouch, Abdulrazzaq Qattea, Wafaa Qatteh, Sami Qattea","doi":"10.1055/s-0045-1801841","DOIUrl":null,"url":null,"abstract":"<p><p>Ovarian torsion is one of the gynecological emergencies and surgical intervention is the standard management for ovarian salvage as well as reveals some unexpected anatomical defects that increase the risk of ovarian torsion. We report a case of a 27-year-old single, nulliparous female taken for diagnostic laparoscopy with suspicion of ovarian torsion. Intraoperatively, we found right adnexa torsion (ovary with tube) along with incarceration of the right ovary and tube into the big peritoneal sac, which was located medial to the right uterosacral ligament. Detorsion and careful pulling of the swollen adnexa were done to the outside of the big peritoneal sac using nontraumatic laparoscopic forceps. The left side was normal with normal left adnexa. The patient had a second laparoscopic look with a plan for peritoneal closure of the big peritoneal defect. There are two cases which have previously reported ovarian incarceration, but were not associated with ovarian torsion, and did not involve peritoneal closure unlike our report of ovarian detorsion and peritoneal defect closure. The etiology of this condition is thought to be likely congenital as there were no other visible etiologies like pelvic trauma, previous surgery, pelvic inflammatory disease, or endometriosis. Our clinical assessment suggests that a peritoneal sac can enhance the course of ovarian torsion to involve ischemic changes of the ovary when trapped inside of it, by its prevention of spontaneous detorsion. This condition will result in the compression of the cells between the sac wall and subsequent tissue edema enhancing the ischemic effect.</p>","PeriodicalId":32889,"journal":{"name":"Avicenna Journal of Medicine","volume":"14 4","pages":"223-227"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11896718/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Avicenna Journal of Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0045-1801841","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
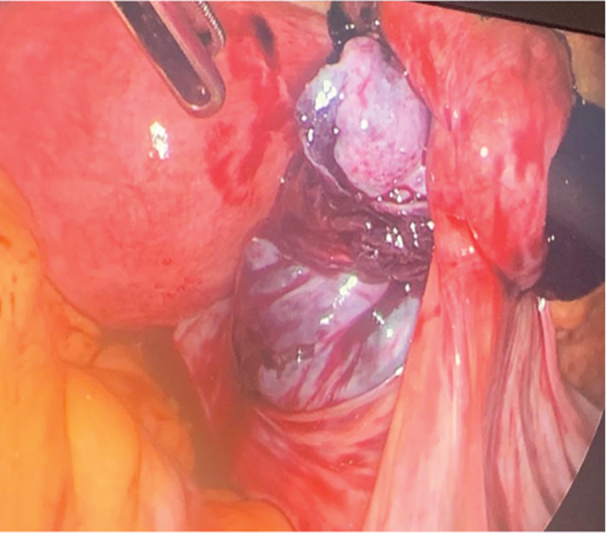
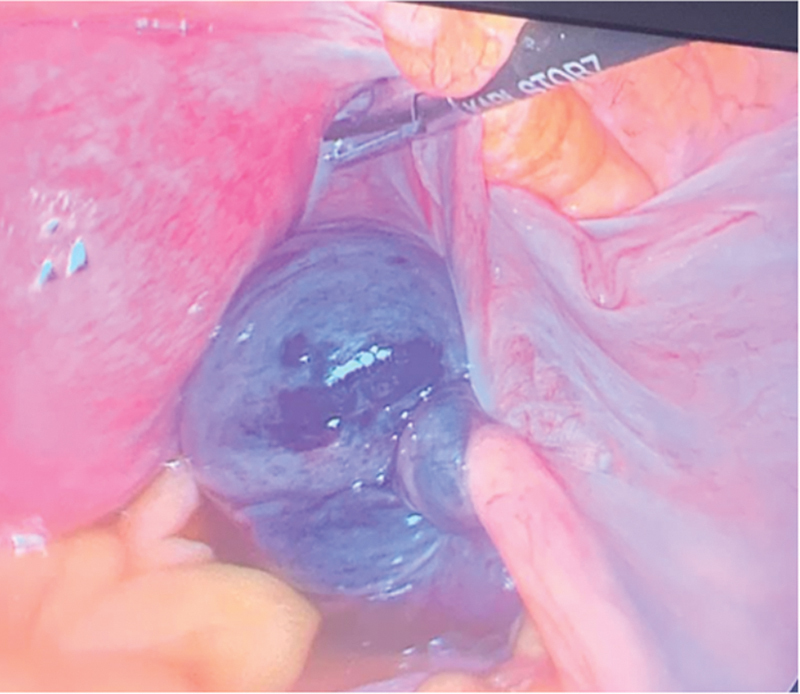
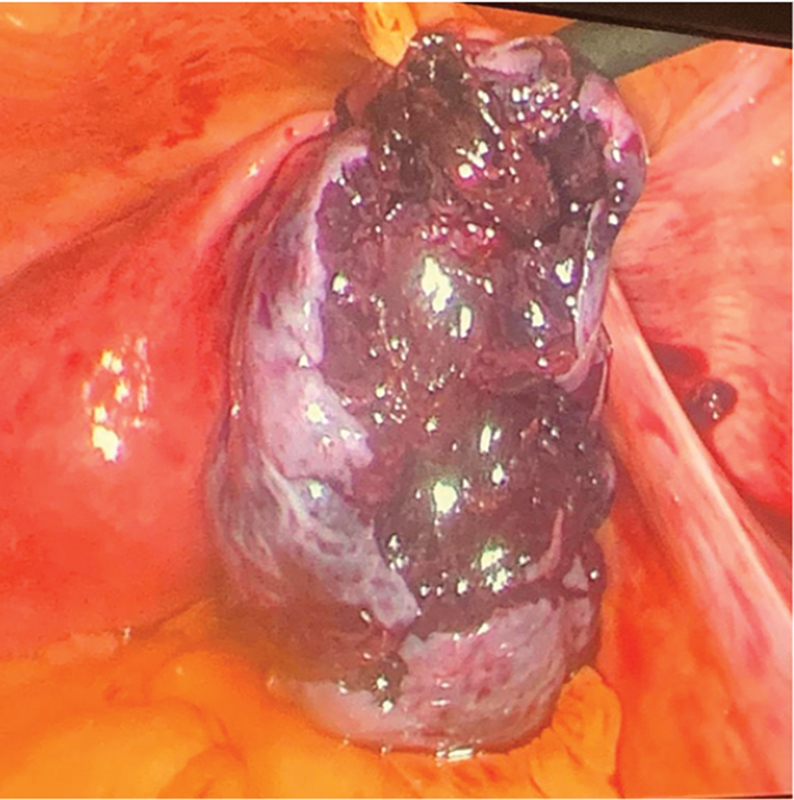
Ovarian torsion is one of the gynecological emergencies and surgical intervention is the standard management for ovarian salvage as well as reveals some unexpected anatomical defects that increase the risk of ovarian torsion. We report a case of a 27-year-old single, nulliparous female taken for diagnostic laparoscopy with suspicion of ovarian torsion. Intraoperatively, we found right adnexa torsion (ovary with tube) along with incarceration of the right ovary and tube into the big peritoneal sac, which was located medial to the right uterosacral ligament. Detorsion and careful pulling of the swollen adnexa were done to the outside of the big peritoneal sac using nontraumatic laparoscopic forceps. The left side was normal with normal left adnexa. The patient had a second laparoscopic look with a plan for peritoneal closure of the big peritoneal defect. There are two cases which have previously reported ovarian incarceration, but were not associated with ovarian torsion, and did not involve peritoneal closure unlike our report of ovarian detorsion and peritoneal defect closure. The etiology of this condition is thought to be likely congenital as there were no other visible etiologies like pelvic trauma, previous surgery, pelvic inflammatory disease, or endometriosis. Our clinical assessment suggests that a peritoneal sac can enhance the course of ovarian torsion to involve ischemic changes of the ovary when trapped inside of it, by its prevention of spontaneous detorsion. This condition will result in the compression of the cells between the sac wall and subsequent tissue edema enhancing the ischemic effect.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


