Rayaan Rauf, Cheryl A Gibson, Mohamad Alhoda Mohamad Alahmad
{"title":"Impact of Frailty on Inpatient Mortality and Resource Utilization for Primary Pulmonary Hypertension.","authors":"Rayaan Rauf, Cheryl A Gibson, Mohamad Alhoda Mohamad Alahmad","doi":"10.1055/s-0044-1801349","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background</b> Frailty has been associated with inferior outcomes in patients with primary pulmonary hypertension (PPH). There is a lack of national data to assess if hospital frailty risk score (HFRS) is associated with worse inpatient outcomes in PPH. <b>Methods</b> Our retrospective study used the Nationwide Readmission Database (NRD). First, we extracted all cases older than 18 years who were discharged with a principal diagnosis of PPH between January and November 2016 to 2019 to allow for a 30-day follow-up. Appropriate survey and domain analyses were applied to obtain national estimates using SAS 9.4. <b>Results</b> We identified 4,555 cases. HFRS <5 was present in 56% ( <i>n</i> = 2,555) of the cohort. Patients with an intermediate-to-high frailty risk score (HFRS ≥5) were older than those with a low frailty risk score (HFRS <5), with a mean age of 61 versus 54 years ( <i>p</i> < 0.01), and had slightly fewer women (75 vs. 78%, <i>p</i> = 0.09). Patients with HFRS >5 had a higher prevalence of dementia, depression, diabetes mellitus, malignancy, acute encephalopathy, coagulopathy, heart failure, and chronic (liver and renal) diseases ( <i>p</i> < 0.01). Also, they had higher inpatient mortality during index admission (14 vs. 2%, <i>p</i> < 0.001), and all-cause 30-day readmission rates (38 vs. 33%, <i>p</i> = 0.01). Univariate analysis suggests a positive correlation between the degree of frailty and the odds of inpatient mortality (referenced to HFRS <5). The HFRS 5 to 10 group has an odds ratio (OR) of 5 (95% confidence interval [CI]: 3.3-8), the HFRS 10 to 15 group has an OR of 14 (95% CI: 8-23), and the HFRS >15 group has an OR of 20 (95% CI: 9-45). Even after adjusting for age, gender, and significant comorbidities, the single most important factor associated with higher odds of inpatient mortality was HFRS >5 (OR: 5.5 [95% CI: 3.7-8.3], <i>p</i> < 0.001) followed by acute myocardial infarction, acute encephalopathy, heart failure, chronic liver disease, and malnutrition. Length of stay had linear trend with HFRS (mean of 6 days for HFRS <5 vs. 11 days for HFRS 5-10 vs. 19 days for HFRS >10, <i>p</i> < 0.001). <b>Conclusion</b> Adverse inpatient outcomes correlate with the severity of HFRS in PPH.</p>","PeriodicalId":32889,"journal":{"name":"Avicenna Journal of Medicine","volume":"14 4","pages":"204-209"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11896733/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Avicenna Journal of Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0044-1801349","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
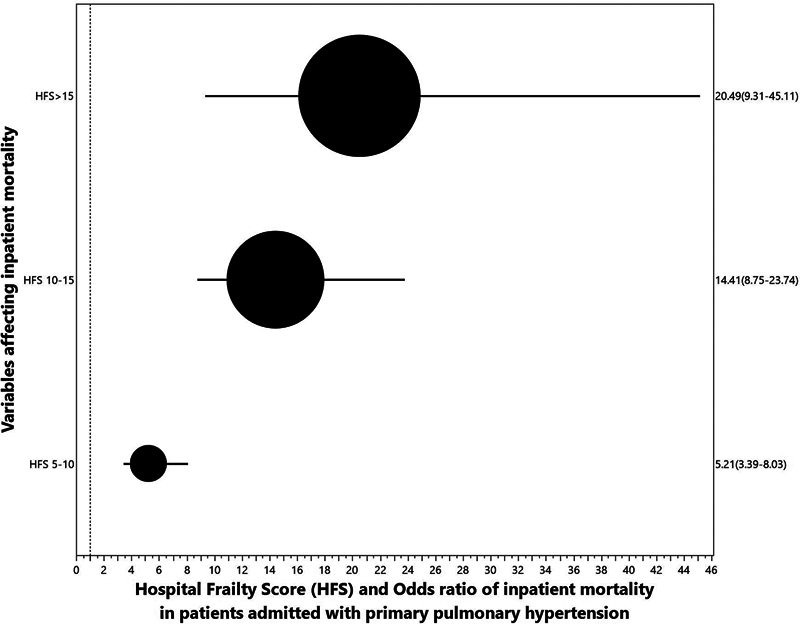
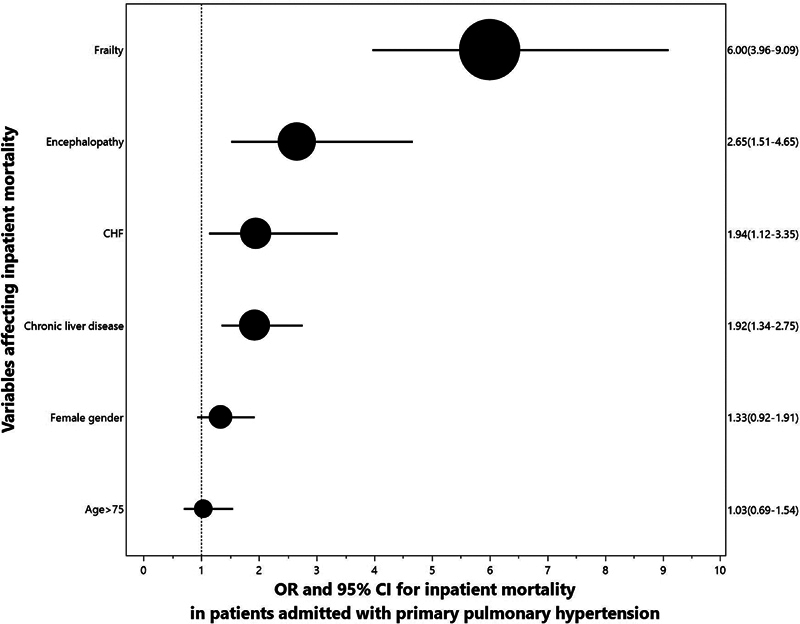
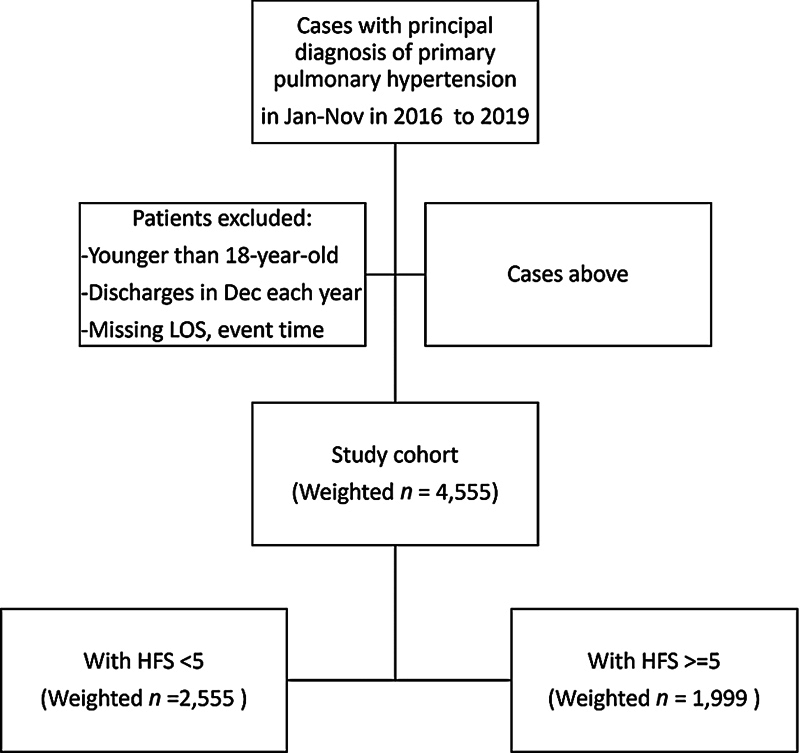
Background Frailty has been associated with inferior outcomes in patients with primary pulmonary hypertension (PPH). There is a lack of national data to assess if hospital frailty risk score (HFRS) is associated with worse inpatient outcomes in PPH. Methods Our retrospective study used the Nationwide Readmission Database (NRD). First, we extracted all cases older than 18 years who were discharged with a principal diagnosis of PPH between January and November 2016 to 2019 to allow for a 30-day follow-up. Appropriate survey and domain analyses were applied to obtain national estimates using SAS 9.4. Results We identified 4,555 cases. HFRS <5 was present in 56% ( n = 2,555) of the cohort. Patients with an intermediate-to-high frailty risk score (HFRS ≥5) were older than those with a low frailty risk score (HFRS <5), with a mean age of 61 versus 54 years ( p < 0.01), and had slightly fewer women (75 vs. 78%, p = 0.09). Patients with HFRS >5 had a higher prevalence of dementia, depression, diabetes mellitus, malignancy, acute encephalopathy, coagulopathy, heart failure, and chronic (liver and renal) diseases ( p < 0.01). Also, they had higher inpatient mortality during index admission (14 vs. 2%, p < 0.001), and all-cause 30-day readmission rates (38 vs. 33%, p = 0.01). Univariate analysis suggests a positive correlation between the degree of frailty and the odds of inpatient mortality (referenced to HFRS <5). The HFRS 5 to 10 group has an odds ratio (OR) of 5 (95% confidence interval [CI]: 3.3-8), the HFRS 10 to 15 group has an OR of 14 (95% CI: 8-23), and the HFRS >15 group has an OR of 20 (95% CI: 9-45). Even after adjusting for age, gender, and significant comorbidities, the single most important factor associated with higher odds of inpatient mortality was HFRS >5 (OR: 5.5 [95% CI: 3.7-8.3], p < 0.001) followed by acute myocardial infarction, acute encephalopathy, heart failure, chronic liver disease, and malnutrition. Length of stay had linear trend with HFRS (mean of 6 days for HFRS <5 vs. 11 days for HFRS 5-10 vs. 19 days for HFRS >10, p < 0.001). Conclusion Adverse inpatient outcomes correlate with the severity of HFRS in PPH.
背景:原发性肺动脉高压(PPH)患者虚弱与预后不良相关。目前缺乏国家数据来评估医院虚弱风险评分(HFRS)是否与PPH住院预后较差相关。方法采用全国再入院数据库(NRD)进行回顾性研究。首先,我们提取了2016年1月至11月至2019年期间以PPH主要诊断出院的所有年龄大于18岁的病例,以便进行30天的随访。使用SAS 9.4进行适当的调查和领域分析以获得全国估计数。结果共发现4555例病例。HFRS n = 2555)。中高衰弱风险评分(HFRS≥5)的患者比低衰弱风险评分的患者年龄大(HFRS p p = 0.09)。HFRS bbbb5患者痴呆、抑郁、糖尿病、恶性肿瘤、急性脑病、凝血功能障碍、心力衰竭和慢性(肝脏和肾脏)疾病的患病率较高(p p p = 0.01)。单因素分析表明,虚弱程度与住院死亡率之间存在正相关(参考HFRS 15组,OR为20 (95% CI: 9-45)。即使在调整了年龄、性别和显著合并症后,与住院患者死亡率较高的几率相关的最重要因素是HFRS bb0.5 (OR: 5.5 [95% CI: 3.7-8.3], p 10, p)。结论:PPH患者的不良住院结果与HFRS的严重程度相关。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


