Xiaoming Bao, Kun Ren, Weidong Guo, Xiaoping Zhang, Xin Dong, Kang Yan, Huanhuan Qiao, Haien Zhao, Bo Liao
{"title":"Comparison of Anterior Surgery Versus Posterior Surgery for the Treatment of Multilevel Cervical Spondylotic Myelopathy: A Meta-Analysis.","authors":"Xiaoming Bao, Kun Ren, Weidong Guo, Xiaoping Zhang, Xin Dong, Kang Yan, Huanhuan Qiao, Haien Zhao, Bo Liao","doi":"10.1097/BSD.0000000000001778","DOIUrl":null,"url":null,"abstract":"<p><strong>Study design: </strong>A meta-analysis.</p><p><strong>Objective: </strong>To evaluate the impact of anterior versus posterior surgical approaches on outcomes in MCSM.</p><p><strong>Background: </strong>Multilevel cervical spondylotic myelopathy (MCSM) is the most common cause of spinal cord dysfunction, and the clinical effectiveness of anterior versus posterior surgical approaches remains elusive.</p><p><strong>Methods: </strong>A comprehensive search was conducted across electronic databases, including MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials, to evaluate the effects of anterior surgery versus posterior surgery on outcomes, such as Japanese Orthopedic Association (JOA) score, neck disability index (NDI) score, neck visual analog scale (VAS), blood loss, operation time, length of stay, cervical range of motion, cervical Cobb angle, and complications. The baseline characteristics of the included studies were assessed using the Newcastle-Ottawa Scale score to measure the risk of bias.</p><p><strong>Results: </strong>In this meta-analysis, 14 retrospective and 6 prospective cohort studies, involving 2712 patients, were included. The analysis indicated no significant difference between the 2 groups in preoperative JOA score, postoperative JOA score, JOA recovery rate, postoperative neck VAS score, operation time, preoperative range of motion (ROM), or SF-36 score ( P =0.95, 0.15, 0.20, 0.31, 0.94, 0.33, and 0.43, respectively). However, the NDI score and blood loss were significantly lower in the anterior surgery group compared with the posterior surgery group ( P <0.04, P =0.0003). The anterior surgery group was also associated with shorter length of stay ( P <0.00001), while had higher rates of complications ( P =0.04). C2-7 Cobb angle and postoperative ROM were significantly lower in the anterior surgery group than those in the posterior surgery group ( P =0.0002 and 0.01, respectively).</p><p><strong>Conclusion: </strong>This meta-analysis found no clear advantage of 1 surgical approach over the other for MCSM in terms of neurological function recovery, as measured by JOA scores. The anterior approach was associated with improved NDI scores, lower blood loss, shorter length of stay, and better recovery of cervical lordosis, accompanied by limited postoperative mobility. Careful consideration should be given to potential complications, including dysphagia with the anterior surgery, axial pain, and C5 palsy with the posterior surgery.</p>","PeriodicalId":10457,"journal":{"name":"Clinical Spine Surgery","volume":" ","pages":"333-344"},"PeriodicalIF":1.7000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12278754/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Spine Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/BSD.0000000000001778","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/13 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Study design: A meta-analysis.
Objective: To evaluate the impact of anterior versus posterior surgical approaches on outcomes in MCSM.
Background: Multilevel cervical spondylotic myelopathy (MCSM) is the most common cause of spinal cord dysfunction, and the clinical effectiveness of anterior versus posterior surgical approaches remains elusive.
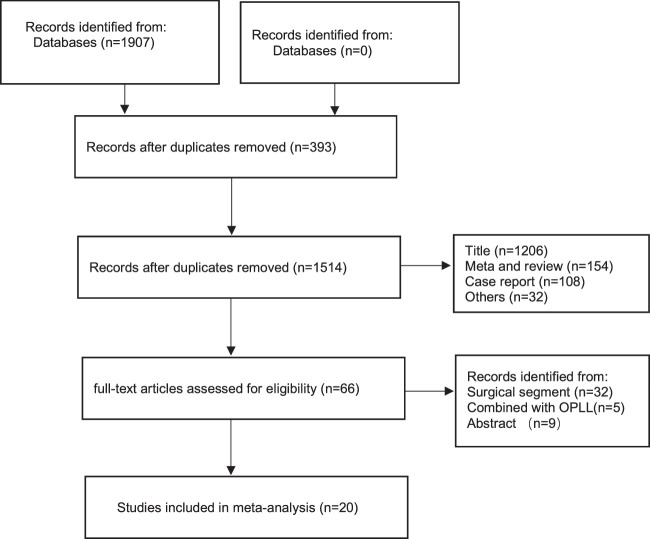
Methods: A comprehensive search was conducted across electronic databases, including MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials, to evaluate the effects of anterior surgery versus posterior surgery on outcomes, such as Japanese Orthopedic Association (JOA) score, neck disability index (NDI) score, neck visual analog scale (VAS), blood loss, operation time, length of stay, cervical range of motion, cervical Cobb angle, and complications. The baseline characteristics of the included studies were assessed using the Newcastle-Ottawa Scale score to measure the risk of bias.
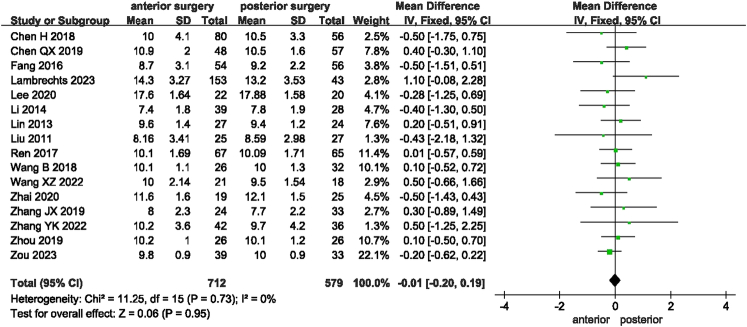
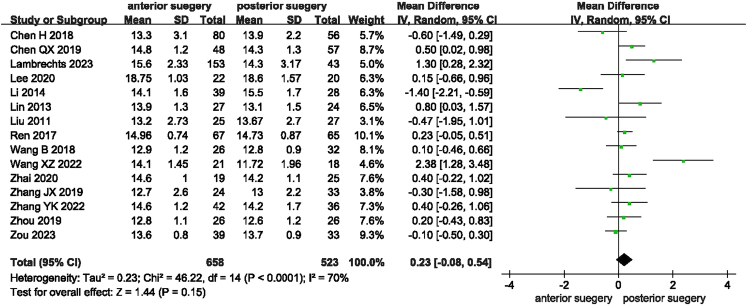
Results: In this meta-analysis, 14 retrospective and 6 prospective cohort studies, involving 2712 patients, were included. The analysis indicated no significant difference between the 2 groups in preoperative JOA score, postoperative JOA score, JOA recovery rate, postoperative neck VAS score, operation time, preoperative range of motion (ROM), or SF-36 score ( P =0.95, 0.15, 0.20, 0.31, 0.94, 0.33, and 0.43, respectively). However, the NDI score and blood loss were significantly lower in the anterior surgery group compared with the posterior surgery group ( P <0.04, P =0.0003). The anterior surgery group was also associated with shorter length of stay ( P <0.00001), while had higher rates of complications ( P =0.04). C2-7 Cobb angle and postoperative ROM were significantly lower in the anterior surgery group than those in the posterior surgery group ( P =0.0002 and 0.01, respectively).
Conclusion: This meta-analysis found no clear advantage of 1 surgical approach over the other for MCSM in terms of neurological function recovery, as measured by JOA scores. The anterior approach was associated with improved NDI scores, lower blood loss, shorter length of stay, and better recovery of cervical lordosis, accompanied by limited postoperative mobility. Careful consideration should be given to potential complications, including dysphagia with the anterior surgery, axial pain, and C5 palsy with the posterior surgery.
期刊介绍:
Clinical Spine Surgery is the ideal journal for the busy practicing spine surgeon or trainee, as it is the only journal necessary to keep up to date with new clinical research and surgical techniques. Readers get to watch leaders in the field debate controversial topics in a new controversies section, and gain access to evidence-based reviews of important pathologies in the systematic reviews section. The journal features a surgical technique complete with a video, and a tips and tricks section that allows surgeons to review the important steps prior to a complex procedure.
Clinical Spine Surgery provides readers with primary research studies, specifically level 1, 2 and 3 studies, ensuring that articles that may actually change a surgeon’s practice will be read and published. Each issue includes a brief article that will help a surgeon better understand the business of healthcare, as well as an article that will help a surgeon understand how to interpret increasingly complex research methodology. Clinical Spine Surgery is your single source for up-to-date, evidence-based recommendations for spine care.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


