Low-density lipoprotein cholesterol levels and treatment intensity in secondary prevention of patients with ischaemic heart disease in the primary care setting: a real-world data registry study.
Núria Sánchez-Ruano, Anna Fibla-Matamoros, Carles Falces, Encarna Sánchez, Antoni Sisó-Almirall, Luis González-de Paz
{"title":"Low-density lipoprotein cholesterol levels and treatment intensity in secondary prevention of patients with ischaemic heart disease in the primary care setting: a real-world data registry study.","authors":"Núria Sánchez-Ruano, Anna Fibla-Matamoros, Carles Falces, Encarna Sánchez, Antoni Sisó-Almirall, Luis González-de Paz","doi":"10.3399/BJGPO.2024.0220","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Monitoring low-density lipoprotein cholesterol (LDL-C) and prescribing appropriate treatment is crucial for secondary prevention in primary care.</p><p><strong>Aim: </strong>To study LDL-C levels and treatments for patients with ischaemic heart disease according to target recommendations and assess factors influencing prescribed drug intensity.</p><p><strong>Design & setting: </strong>A cross-sectional study was undertaken. We examined electronic health records of patients with ischaemic heart disease from three primary care centres in Spain.</p><p><strong>Method: </strong>LDL-C levels were assessed using the most recent registry, and LDL-C-lowering treatments were categorised by their theoretical efficacy. Factors associated with LDL-C target attainment were analysed using univariate and multivariate regression models. Prescription intensity was studied with ordinal logistic regression models.</p><p><strong>Results: </strong>We studied 1936 patients, 14.88% of whom received no LDL-C-lowering treatment. The percentages of patients who achieved LDL-C thresholds of<70 mg/dl and<55 mg/dl were 35.0% and 12.65%, respectively. The factor associated with the <55 mg/dl threshold was type 2 diabetes mellitus (odds ratio [OR] 0.55, 95% confidence interval [CI] = 0.42 to 0.73), with males showing better LDL-C levels (OR 0.34, 95% CI = 0.23 to 0.51). Males had higher-intensity prescriptions (OR 1.57, 95% CI = 1.27 to 1.94) and older patients had lower-intensity treatments (OR 0.96, 95% CI = 0.95 to 0.97).</p><p><strong>Conclusion: </strong>Increased LDL-C drug treatment improvement, monitoring, and adherence to guideline recommendations are necessary for patients with ischaemic heart disease. Sex and age are potential factors associated with inadequate lipid-lowering treatment intensity and poor LDL-C control that might worsen cardiovascular outcomes in high-risk patients, leading to avoidable inequity among patients who visit the primary health setting.</p>","PeriodicalId":36541,"journal":{"name":"BJGP Open","volume":" ","pages":""},"PeriodicalIF":2.0000,"publicationDate":"2025-07-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12421263/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJGP Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3399/BJGPO.2024.0220","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"Print","JCR":"Q2","JCRName":"PRIMARY HEALTH CARE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Monitoring low-density lipoprotein cholesterol (LDL-C) and prescribing appropriate treatment is crucial for secondary prevention in primary care.
Aim: To study LDL-C levels and treatments for patients with ischaemic heart disease according to target recommendations and assess factors influencing prescribed drug intensity.
Design & setting: A cross-sectional study was undertaken. We examined electronic health records of patients with ischaemic heart disease from three primary care centres in Spain.
Method: LDL-C levels were assessed using the most recent registry, and LDL-C-lowering treatments were categorised by their theoretical efficacy. Factors associated with LDL-C target attainment were analysed using univariate and multivariate regression models. Prescription intensity was studied with ordinal logistic regression models.
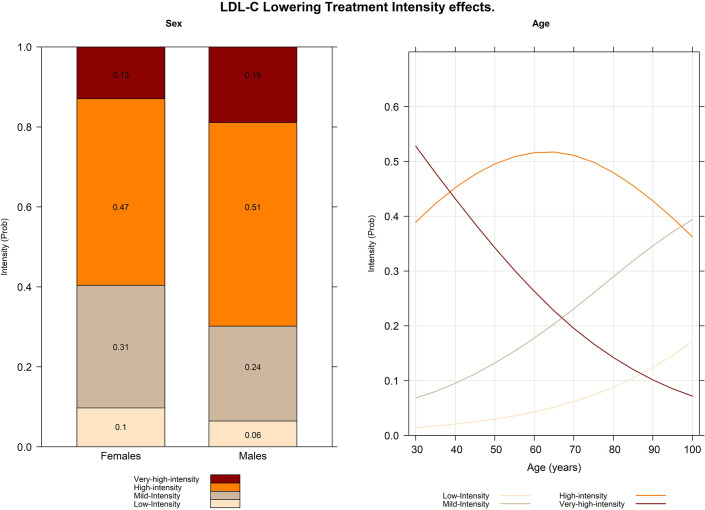
Results: We studied 1936 patients, 14.88% of whom received no LDL-C-lowering treatment. The percentages of patients who achieved LDL-C thresholds of<70 mg/dl and<55 mg/dl were 35.0% and 12.65%, respectively. The factor associated with the <55 mg/dl threshold was type 2 diabetes mellitus (odds ratio [OR] 0.55, 95% confidence interval [CI] = 0.42 to 0.73), with males showing better LDL-C levels (OR 0.34, 95% CI = 0.23 to 0.51). Males had higher-intensity prescriptions (OR 1.57, 95% CI = 1.27 to 1.94) and older patients had lower-intensity treatments (OR 0.96, 95% CI = 0.95 to 0.97).
Conclusion: Increased LDL-C drug treatment improvement, monitoring, and adherence to guideline recommendations are necessary for patients with ischaemic heart disease. Sex and age are potential factors associated with inadequate lipid-lowering treatment intensity and poor LDL-C control that might worsen cardiovascular outcomes in high-risk patients, leading to avoidable inequity among patients who visit the primary health setting.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


