Suzanna Larkin, Brooke W Bullington, Kristen A Berg, Kari White, Margaret Boozer, Tania Serna, Emily S Miller, Jennifer L Bailit, Kavita Shah Arora
{"title":"Multi-level barriers to equitable postpartum permanent contraception.","authors":"Suzanna Larkin, Brooke W Bullington, Kristen A Berg, Kari White, Margaret Boozer, Tania Serna, Emily S Miller, Jennifer L Bailit, Kavita Shah Arora","doi":"10.1177/17455057251325977","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There are several barriers to fulfillment of desired postpartum permanent contraception (PC). Prior research has primarily focused on the federal Medicaid sterilization policy as a barrier to PC; however, other barriers need to be examined.</p><p><strong>Objectives: </strong>To explore the levels and intersections of barriers to postpartum PC that exist external to the Medicaid policy.</p><p><strong>Design: </strong>We interviewed postpartum people with a documented desire for PC and their delivering obstetrician-gynecologist (OB-GYN) at four hospitals in the United States in 2022-2023.</p><p><strong>Methods: </strong>We used rapid qualitative analysis to create initial key themes and sub-themes, which we further refined using thematic analysis to explore barriers to postpartum PC.</p><p><strong>Results: </strong>We interviewed 81 postpartum people and 67 OB-GYNs. Barriers were identified across four levels: clinical, physician, hospital, and sociocultural. At the clinical level, participants commented on how they believed individual patient characteristics and medical history can prevent PC fulfillment prior to discharge. At the physician level, participants discussed young age, low parity, and marital status as reasons clinicians decline to provide desired PC. At the hospital level, OB-GYNs described difficulties with scheduling and staffing, and patients described a lack of PC prioritization. At the sociocultural level, participants mentioned numerous barriers to fulfillment of interval PC including finding childcare, getting appointments scheduled quickly, and transportation.</p><p><strong>Conclusion: </strong>Improving access to postpartum PC should be focused within and across all levels of health disparity determinants. In the cases where immediate PC is not accessible, interventions should be formulated across levels to allow timely access to interval PC. As policy reform alone will not eliminate all barriers to postpartum PC, a multi-level approach to alleviating barriers is required.</p>","PeriodicalId":75327,"journal":{"name":"Women's health (London, England)","volume":"21 ","pages":"17455057251325977"},"PeriodicalIF":2.9000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11905033/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Women's health (London, England)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/17455057251325977","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/12 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: There are several barriers to fulfillment of desired postpartum permanent contraception (PC). Prior research has primarily focused on the federal Medicaid sterilization policy as a barrier to PC; however, other barriers need to be examined.
Objectives: To explore the levels and intersections of barriers to postpartum PC that exist external to the Medicaid policy.
Design: We interviewed postpartum people with a documented desire for PC and their delivering obstetrician-gynecologist (OB-GYN) at four hospitals in the United States in 2022-2023.
Methods: We used rapid qualitative analysis to create initial key themes and sub-themes, which we further refined using thematic analysis to explore barriers to postpartum PC.
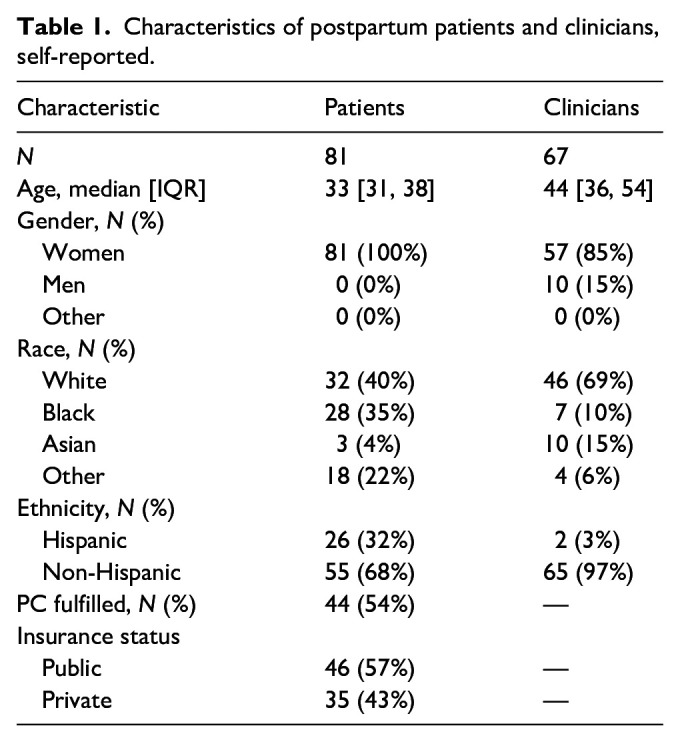
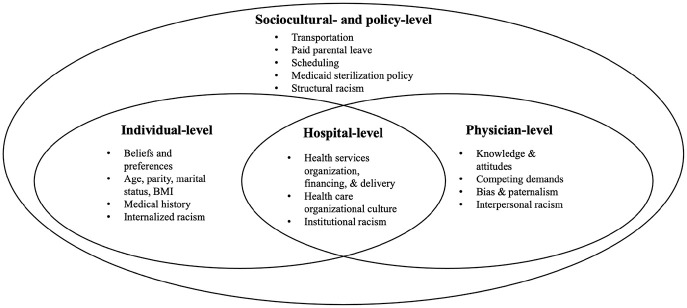
Results: We interviewed 81 postpartum people and 67 OB-GYNs. Barriers were identified across four levels: clinical, physician, hospital, and sociocultural. At the clinical level, participants commented on how they believed individual patient characteristics and medical history can prevent PC fulfillment prior to discharge. At the physician level, participants discussed young age, low parity, and marital status as reasons clinicians decline to provide desired PC. At the hospital level, OB-GYNs described difficulties with scheduling and staffing, and patients described a lack of PC prioritization. At the sociocultural level, participants mentioned numerous barriers to fulfillment of interval PC including finding childcare, getting appointments scheduled quickly, and transportation.
Conclusion: Improving access to postpartum PC should be focused within and across all levels of health disparity determinants. In the cases where immediate PC is not accessible, interventions should be formulated across levels to allow timely access to interval PC. As policy reform alone will not eliminate all barriers to postpartum PC, a multi-level approach to alleviating barriers is required.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


