Valérie M Smit-Fun, Dianne de Korte-de Boer, Thomas Damen, Annick Stolze, Linda M Posthuma, Markus W Hollmann, Wolfgang F F A Buhre
{"title":"Routine anaesthesia ward-based patient visits in surgery: 1-year outcomes of the TRACE randomized clinical trial.","authors":"Valérie M Smit-Fun, Dianne de Korte-de Boer, Thomas Damen, Annick Stolze, Linda M Posthuma, Markus W Hollmann, Wolfgang F F A Buhre","doi":"10.1093/bjs/znaf019","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The TRACE (Routine posTsuRgical Anaesthesia visit to improve patient outComE) RCT did not show any perioperative benefit from ward-based visits by anaesthetists after surgery. The aim of this study was to evaluate the impact of this intervention on longer-term outcomes.</p><p><strong>Methods: </strong>Patients were followed up in the TRACE RCT to 1 year in nine hospitals in the Netherlands. Patients undergoing elective non-cardiac surgery, and at risk for adverse postoperative outcome, were included. Patients in the intervention group additionally received routine anaesthesia visits on postoperative days 1 and 3. Clinical outcome measures included 1-year mortality, hospital readmission, and reoperation. Functional recovery (FR) was measured using the patient-reported global surgical recovery (GSR) index, ability to perform activities of daily living (ADL), and functional recovery index (FRI). Quality of life (QoL) was measured using EQ-5D-5L.</p><p><strong>Results: </strong>Some 5473 adult patients were followed up. No differences were found between the control and intervention groups for clinical, FR, and QoL outcome measures. One-year mortality was 5.4% in the control group and 5.8% in the intervention group, readmission was 27% and 26% respectively, and reoperation was 20% and 18% respectively. At 1 year, FR and QoL had recovered to preoperative levels. However, 30% of patients were not able to fully perform ADL and 40%-51% of patients still reported a problem in the EQ-5D-5L dimensions mobility, usual activities, and pain/discomfort.</p><p><strong>Conclusion: </strong>Routine postoperative anaesthesia ward visits of patients did not improve clinical, functional, and QoL outcomes. A substantial proportion of patients still experienced health-related limitations in daily life 1 year after surgery. In conclusion, an early postoperative intervention with postoperative anaesthesia visits in the ward after non-cardiac surgery had no effect on 30-day or 1-year clinical outcome. Remarkably, TRACE shows that compared with data sampled 10 years ago, 1-year mortality has not improved in the Netherlands. At 1 year, functional recovery or QoL showed little improvement compared with baseline. Importantly, a substantial number of patients still reported incomplete recovery and problems that limit QoL, which indicate that there is still room for improvement.</p>","PeriodicalId":136,"journal":{"name":"British Journal of Surgery","volume":"112 3","pages":""},"PeriodicalIF":8.8000,"publicationDate":"2025-03-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11897594/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"British Journal of Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/bjs/znaf019","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The TRACE (Routine posTsuRgical Anaesthesia visit to improve patient outComE) RCT did not show any perioperative benefit from ward-based visits by anaesthetists after surgery. The aim of this study was to evaluate the impact of this intervention on longer-term outcomes.
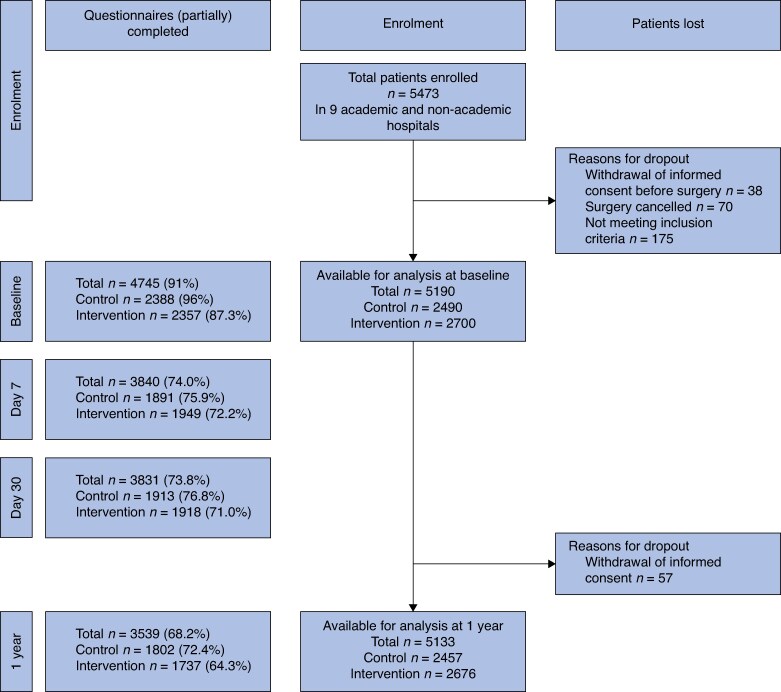
Methods: Patients were followed up in the TRACE RCT to 1 year in nine hospitals in the Netherlands. Patients undergoing elective non-cardiac surgery, and at risk for adverse postoperative outcome, were included. Patients in the intervention group additionally received routine anaesthesia visits on postoperative days 1 and 3. Clinical outcome measures included 1-year mortality, hospital readmission, and reoperation. Functional recovery (FR) was measured using the patient-reported global surgical recovery (GSR) index, ability to perform activities of daily living (ADL), and functional recovery index (FRI). Quality of life (QoL) was measured using EQ-5D-5L.
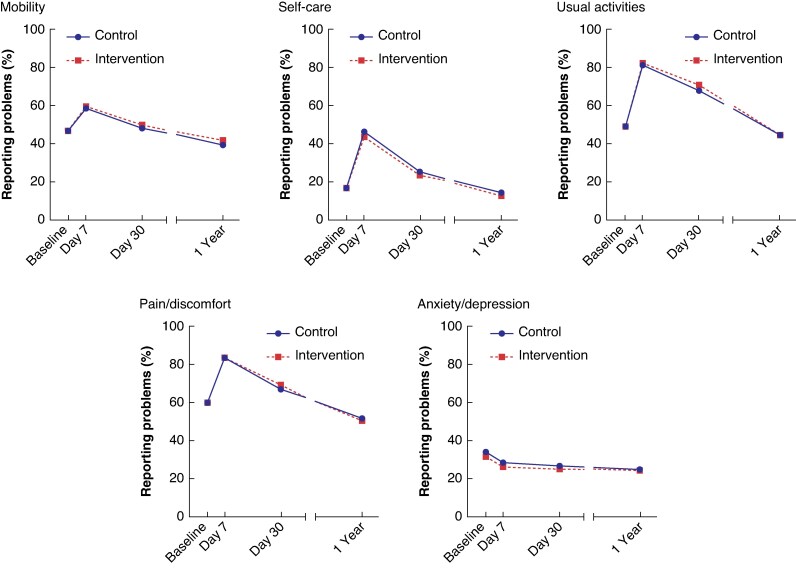
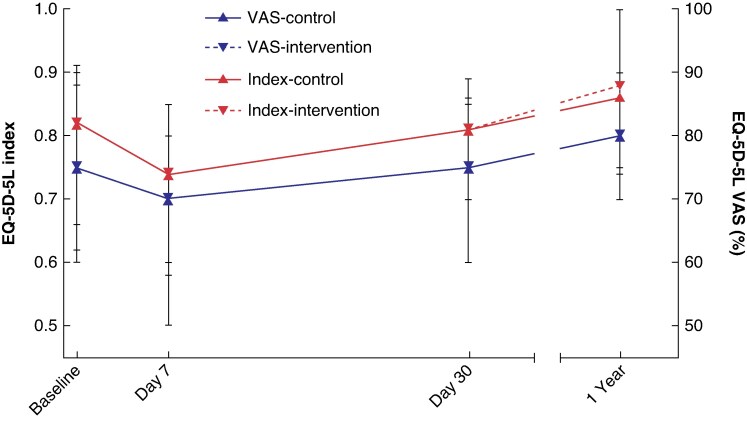
Results: Some 5473 adult patients were followed up. No differences were found between the control and intervention groups for clinical, FR, and QoL outcome measures. One-year mortality was 5.4% in the control group and 5.8% in the intervention group, readmission was 27% and 26% respectively, and reoperation was 20% and 18% respectively. At 1 year, FR and QoL had recovered to preoperative levels. However, 30% of patients were not able to fully perform ADL and 40%-51% of patients still reported a problem in the EQ-5D-5L dimensions mobility, usual activities, and pain/discomfort.
Conclusion: Routine postoperative anaesthesia ward visits of patients did not improve clinical, functional, and QoL outcomes. A substantial proportion of patients still experienced health-related limitations in daily life 1 year after surgery. In conclusion, an early postoperative intervention with postoperative anaesthesia visits in the ward after non-cardiac surgery had no effect on 30-day or 1-year clinical outcome. Remarkably, TRACE shows that compared with data sampled 10 years ago, 1-year mortality has not improved in the Netherlands. At 1 year, functional recovery or QoL showed little improvement compared with baseline. Importantly, a substantial number of patients still reported incomplete recovery and problems that limit QoL, which indicate that there is still room for improvement.
期刊介绍:
The British Journal of Surgery (BJS), incorporating the European Journal of Surgery, stands as Europe's leading peer-reviewed surgical journal. It serves as an invaluable platform for presenting high-quality clinical and laboratory-based research across a wide range of surgical topics. In addition to providing a comprehensive coverage of traditional surgical practices, BJS also showcases emerging areas in the field, such as minimally invasive therapy and interventional radiology.
While the journal appeals to general surgeons, it also holds relevance for specialty surgeons and professionals working in closely related fields. By presenting cutting-edge research and advancements, BJS aims to revolutionize the way surgical knowledge is shared and contribute to the ongoing progress of the surgical community.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


