{"title":"Congenital anomalies of coronary artery misdiagnosed as coronary dilatations in Kawasaki disease: A clinical predicament.","authors":"Rakesh Kumar Pilania, Pallavi L Nadig, Suprit Basu, Reva Tyagi, Abarna Thangaraj, Ridhima Aggarwal, Munish Arora, Arun Sharma, Surjit Singh, Manphool Singhal","doi":"10.5409/wjcp.v14.i1.99177","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>2D-echocardiography (2DE) has been the primary imaging modality in children with Kawasaki disease (KD) to assess coronary arteries.</p><p><strong>Aim: </strong>To report the presence and implications of incidental congenital coronary artery anomalies that had been misinterpreted as coronary artery abnormalities (CAAs) on 2DE.</p><p><strong>Methods: </strong>Records of children diagnosed with KD, who underwent computed tomography coronary angiography (CTCA) at our center between 2013-2023 were reviewed. We identified 3 children with congenital coronary artery anomalies in this cohort on CTCA. Findings of CTCA and 2DE were compared in these 3 children.</p><p><strong>Results: </strong>Of the 241 patients with KD who underwent CTCA, 3 (1.24%) had congenital coronary artery anomalies on CTCA detected incidentally. In all 3 patients, baseline 2DE had identified CAAs. CTCA was then performed for detailed evaluation as per our unit protocol. One (11-year-boy) amongst the 3 patients had complete KD, while the other two (3.3-year-boy; 4-month-girl) had incomplete KD. CTCA revealed separate origins of left anterior descending artery and left circumflex from left sinus [misinterpreted as dilated left main coronary artery (LCA) on 2DE], single coronary artery (interpreted as dilated LCA on 2DE) and dilated right coronary artery on 2DE in case of anomalous origin of LCA from the main pulmonary artery. The latter one was subsequently operated upon.</p><p><strong>Conclusion: </strong>CTCA is essential for detailed assessment of coronary arteries in children with KD especially in cases where there is suspicion of congenital coronary artery anomalies. Relying solely on 2DE may not be sufficient in such cases, and findings from CTCA can significantly impact therapeutic decision-making.</p>","PeriodicalId":75338,"journal":{"name":"World journal of clinical pediatrics","volume":"14 1","pages":"99177"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11686587/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World journal of clinical pediatrics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5409/wjcp.v14.i1.99177","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: 2D-echocardiography (2DE) has been the primary imaging modality in children with Kawasaki disease (KD) to assess coronary arteries.
Aim: To report the presence and implications of incidental congenital coronary artery anomalies that had been misinterpreted as coronary artery abnormalities (CAAs) on 2DE.
Methods: Records of children diagnosed with KD, who underwent computed tomography coronary angiography (CTCA) at our center between 2013-2023 were reviewed. We identified 3 children with congenital coronary artery anomalies in this cohort on CTCA. Findings of CTCA and 2DE were compared in these 3 children.
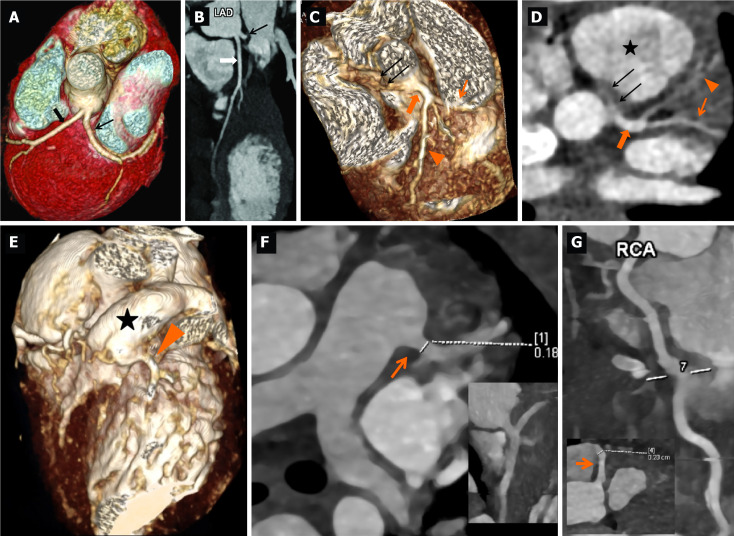
Results: Of the 241 patients with KD who underwent CTCA, 3 (1.24%) had congenital coronary artery anomalies on CTCA detected incidentally. In all 3 patients, baseline 2DE had identified CAAs. CTCA was then performed for detailed evaluation as per our unit protocol. One (11-year-boy) amongst the 3 patients had complete KD, while the other two (3.3-year-boy; 4-month-girl) had incomplete KD. CTCA revealed separate origins of left anterior descending artery and left circumflex from left sinus [misinterpreted as dilated left main coronary artery (LCA) on 2DE], single coronary artery (interpreted as dilated LCA on 2DE) and dilated right coronary artery on 2DE in case of anomalous origin of LCA from the main pulmonary artery. The latter one was subsequently operated upon.
Conclusion: CTCA is essential for detailed assessment of coronary arteries in children with KD especially in cases where there is suspicion of congenital coronary artery anomalies. Relying solely on 2DE may not be sufficient in such cases, and findings from CTCA can significantly impact therapeutic decision-making.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


