{"title":"Integrated Pediatric Intensive Care and Hematopoietic Stem Cell Transplantation Service Improves The Peri-Transplant Survival In Children.","authors":"Nalla Anuraag Reddy, Rachit Mehta, Indira Jayakumar, Anupama Nair, Vijayshree Muthukumar, Suresh Duraisamy, Venkateswaran Vellaichamy Swaminathan, Ramya Uppuluri, Revathi Raj","doi":"10.31547/bct-2024-014","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Peri-transplant is a critical period which is associated with a myriad of complications that require pediatric intensive care unit (PICU) referral. PICU outcomes have been historically poor post-hematopoietic stem cell transplantation (HSCT), especially when associated with inotrope support, invasive ventilation, and renal replacement therapy. The study aimed to assess the outcomes of PICU referral in children undergoing HSCT.</p><p><strong>Patients & methods: </strong>A retrospective analysis was performed of children between 1 to 18 years of age who underwent HSCT between 2016 to 2023. A clinical deteriorating event (CDE) was defined as an unplanned transfer to the intensive care unit (ICU) or requiring ICU-level intervention on the floor. The reason for PICU referral, place of intervention, cause for the CDE, and requirement of respiratory, renal, and cardiac support were noted. The study period was divided into two 4-year intervals to assess change over time, 2016-2019 and 2020-2023.</p><p><strong>Results: </strong>In an eight-year period, a total of 934 HSCTs were performed, with 272 patients requiring PICU referral. A total of 415 CDEs were recorded. CDEs for PICU referrals were hypotension (43%), disproportionate tachycardia (42%), respiratory distress (26%), hypertension (22%), altered sensorium (8%), seizures (7.4%), and major bleeds (7.3%). Overall peri-transplant survival was 73.8% (n=201/272). Comparing the two study intervals, 2016-2019 and 2020-2023, the survival of patients on mechanical ventilation had improved from 4.5% to 27.5% (<i>p</i>=0.005) and from 39.4% to 55.9% (<i>p</i>=0.11) among those who received inotropes. Patients with three organ dysfunctions had worse outcomes. Disproportionate tachycardia [OR 0.19 CI 95% (0.06-0.64); <i>p</i>=0.008], hypotension [OR 0.177 CI 95% (0.04-0.84); <i>p</i>=0.029] and acute GVHD [OR 28.46 CI 95% (3.66-221); <i>p</i>=0.001] were significant risk factors for peri-transplant mortality as per multivariate analysis.</p><p><strong>Conclusion: </strong>Integrated care with the PICU team is the first step towards improving survival in these critically ill children. With timely intervention on the floors for CDEs and protocol-driven care in the PICU, we have demonstrated an increase in overall survival over the past four years and would recommend similar team-based care for units catering to children.</p>","PeriodicalId":72423,"journal":{"name":"Blood cell therapy","volume":"8 1","pages":"173-180"},"PeriodicalIF":0.0000,"publicationDate":"2025-02-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11883477/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Blood cell therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31547/bct-2024-014","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Peri-transplant is a critical period which is associated with a myriad of complications that require pediatric intensive care unit (PICU) referral. PICU outcomes have been historically poor post-hematopoietic stem cell transplantation (HSCT), especially when associated with inotrope support, invasive ventilation, and renal replacement therapy. The study aimed to assess the outcomes of PICU referral in children undergoing HSCT.
Patients & methods: A retrospective analysis was performed of children between 1 to 18 years of age who underwent HSCT between 2016 to 2023. A clinical deteriorating event (CDE) was defined as an unplanned transfer to the intensive care unit (ICU) or requiring ICU-level intervention on the floor. The reason for PICU referral, place of intervention, cause for the CDE, and requirement of respiratory, renal, and cardiac support were noted. The study period was divided into two 4-year intervals to assess change over time, 2016-2019 and 2020-2023.
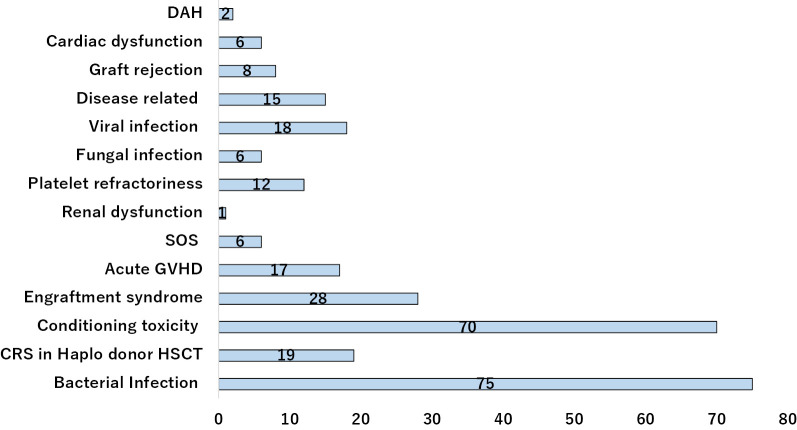
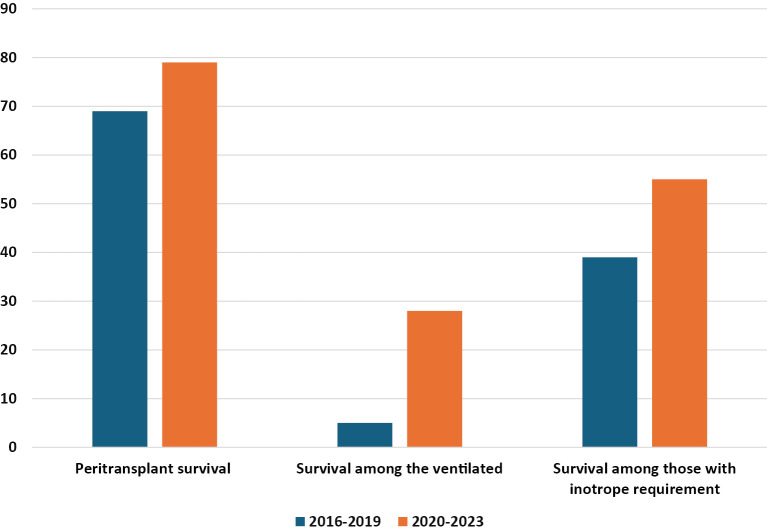
Results: In an eight-year period, a total of 934 HSCTs were performed, with 272 patients requiring PICU referral. A total of 415 CDEs were recorded. CDEs for PICU referrals were hypotension (43%), disproportionate tachycardia (42%), respiratory distress (26%), hypertension (22%), altered sensorium (8%), seizures (7.4%), and major bleeds (7.3%). Overall peri-transplant survival was 73.8% (n=201/272). Comparing the two study intervals, 2016-2019 and 2020-2023, the survival of patients on mechanical ventilation had improved from 4.5% to 27.5% (p=0.005) and from 39.4% to 55.9% (p=0.11) among those who received inotropes. Patients with three organ dysfunctions had worse outcomes. Disproportionate tachycardia [OR 0.19 CI 95% (0.06-0.64); p=0.008], hypotension [OR 0.177 CI 95% (0.04-0.84); p=0.029] and acute GVHD [OR 28.46 CI 95% (3.66-221); p=0.001] were significant risk factors for peri-transplant mortality as per multivariate analysis.
Conclusion: Integrated care with the PICU team is the first step towards improving survival in these critically ill children. With timely intervention on the floors for CDEs and protocol-driven care in the PICU, we have demonstrated an increase in overall survival over the past four years and would recommend similar team-based care for units catering to children.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


