{"title":"Thrombolysis and extracorporeal cardiopulmonary resuscitation for cardiac arrest due to pulmonary embolism: A case report.","authors":"Guan-Xing Yuan, Zhi-Ping Zhang, Jia Zhou","doi":"10.5492/wjccm.v14.i1.97443","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cardiac arrest caused by acute pulmonary embolism (PE) is the most serious clinical circumstance, necessitating rapid identification, immediate cardiopulmonary resuscitation (CPR), and systemic thrombolytic therapy. Extracorporeal CPR (ECPR) is typically employed as a rescue therapy for selected patients when conventional CPR is failing in settings where it can be implemented.</p><p><strong>Case summary: </strong>We present a case of a 69-year-old male who experienced a prolonged cardiac arrest in an ambulance with pulseless electrical activity. Upon arrival at the emergency department with ongoing manual chest compressions, bedside point-of-care ultrasound revealed an enlarged right ventricle without contractility. Acute PE was suspected as the cause of cardiac arrest, and intravenous thrombolytic therapy with 50 mg tissue plasminogen activator was administered during mechanical chest compressions. Despite 31 minutes of CPR, return of spontaneous circulation was not achieved until 8 minutes after initiation of Veno-arterial extracorporeal membrane oxygenation (ECMO) support. Under ECMO support, the hemodynamic status and myocardial contractility significantly improved. However, the patient ultimately did not survive due to intracerebral hemorrhagic complications, leading to death a few days later in the hospital.</p><p><strong>Conclusion: </strong>This case illustrates the potential of combining systemic thrombolysis with ECPR for refractory cardiac arrest caused by acute PE, but it also highlights the increased risk of significant bleeding complications, including fatal intracranial hemorrhage.</p>","PeriodicalId":66959,"journal":{"name":"世界危重病急救学杂志(英文版)","volume":"14 1","pages":"97443"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11671844/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"世界危重病急救学杂志(英文版)","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5492/wjccm.v14.i1.97443","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Cardiac arrest caused by acute pulmonary embolism (PE) is the most serious clinical circumstance, necessitating rapid identification, immediate cardiopulmonary resuscitation (CPR), and systemic thrombolytic therapy. Extracorporeal CPR (ECPR) is typically employed as a rescue therapy for selected patients when conventional CPR is failing in settings where it can be implemented.
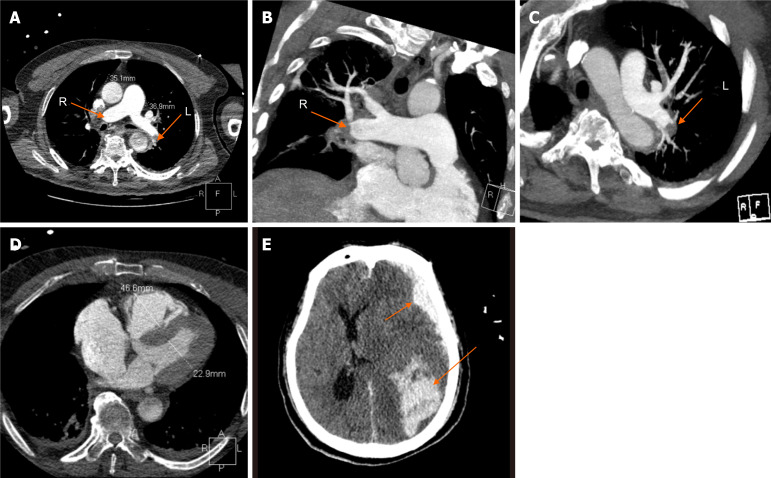
Case summary: We present a case of a 69-year-old male who experienced a prolonged cardiac arrest in an ambulance with pulseless electrical activity. Upon arrival at the emergency department with ongoing manual chest compressions, bedside point-of-care ultrasound revealed an enlarged right ventricle without contractility. Acute PE was suspected as the cause of cardiac arrest, and intravenous thrombolytic therapy with 50 mg tissue plasminogen activator was administered during mechanical chest compressions. Despite 31 minutes of CPR, return of spontaneous circulation was not achieved until 8 minutes after initiation of Veno-arterial extracorporeal membrane oxygenation (ECMO) support. Under ECMO support, the hemodynamic status and myocardial contractility significantly improved. However, the patient ultimately did not survive due to intracerebral hemorrhagic complications, leading to death a few days later in the hospital.
Conclusion: This case illustrates the potential of combining systemic thrombolysis with ECPR for refractory cardiac arrest caused by acute PE, but it also highlights the increased risk of significant bleeding complications, including fatal intracranial hemorrhage.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


