{"title":"Atlantoaxial fixation for treatment of syringobulbia and syringomyelia: Case report and literature review.","authors":"Kaunda Emeka Ibebuike, Oluwamayowa Opara","doi":"10.4103/jcvjs.jcvjs_124_24","DOIUrl":null,"url":null,"abstract":"<p><p>The shunting system has been generally recognized for the treatment of syringomyelia. However, recent publication has documented the role of atlantoaxial stabilization in the treatment of this condition. The objective is to present a case report highlighting our experience in the management of syringobulbia and syringomyelia in an adult male. We present a 45-year-old male who presented with an inability to walk with associated bladder and bowel symptoms. Neuroradiological studies of the brain and the whole spine revealed an extensive syringomyelia extending from the medulla oblongata to the T12 thoracic spinal level. There was no obvious focal mass lesion or bony lesion, and there were no anatomic features suggestive of Chiari I malformation. A management decision was challenging in this case. Atlantoaxial stabilization was considered based on Atul Goel's philosophy that the basic pathology in syringomyelia is C1/C2 instability, and that treatment is C1-C2 fixation. Intraoperative findings confirmed atlantoaxial instability from the direct bone handling during the procedure. There was immediate postoperative improvement in his motor function, which remained sustained, with free and brisk active mobilization at 3 months follow-up. Neuroimaging performed at 14 month's postsurgery revealed a reduction in the size of the syrinx cavity. This single and first experience of atlantoaxial stabilization for the treatment of syringomyelia in our environment may support the assertion by Goel that atlantoaxial instability is the pathology in syringomyelia, and atlantoaxial fixation should be a therapeutic consideration.</p>","PeriodicalId":51721,"journal":{"name":"Journal of Craniovertebral Junction and Spine","volume":"15 4","pages":"506-510"},"PeriodicalIF":1.3000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11888036/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Craniovertebral Junction and Spine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jcvjs.jcvjs_124_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/15 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"OTORHINOLARYNGOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
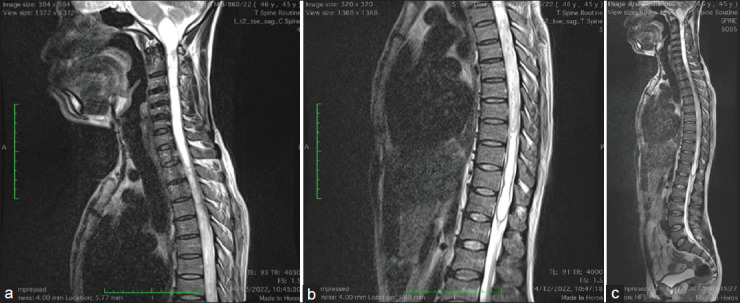
The shunting system has been generally recognized for the treatment of syringomyelia. However, recent publication has documented the role of atlantoaxial stabilization in the treatment of this condition. The objective is to present a case report highlighting our experience in the management of syringobulbia and syringomyelia in an adult male. We present a 45-year-old male who presented with an inability to walk with associated bladder and bowel symptoms. Neuroradiological studies of the brain and the whole spine revealed an extensive syringomyelia extending from the medulla oblongata to the T12 thoracic spinal level. There was no obvious focal mass lesion or bony lesion, and there were no anatomic features suggestive of Chiari I malformation. A management decision was challenging in this case. Atlantoaxial stabilization was considered based on Atul Goel's philosophy that the basic pathology in syringomyelia is C1/C2 instability, and that treatment is C1-C2 fixation. Intraoperative findings confirmed atlantoaxial instability from the direct bone handling during the procedure. There was immediate postoperative improvement in his motor function, which remained sustained, with free and brisk active mobilization at 3 months follow-up. Neuroimaging performed at 14 month's postsurgery revealed a reduction in the size of the syrinx cavity. This single and first experience of atlantoaxial stabilization for the treatment of syringomyelia in our environment may support the assertion by Goel that atlantoaxial instability is the pathology in syringomyelia, and atlantoaxial fixation should be a therapeutic consideration.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


