Krishmita Siwakoti, Allison P Dalton, Jared A Maas, Andrew M McDonald, Samuel R Marcrom, Rex A Cardan, Joseph Harms, John B Fiveash, Adam J Kole
{"title":"Application of Photon-Derived Worst-Case Robustness Criteria to Proton Therapy Planning.","authors":"Krishmita Siwakoti, Allison P Dalton, Jared A Maas, Andrew M McDonald, Samuel R Marcrom, Rex A Cardan, Joseph Harms, John B Fiveash, Adam J Kole","doi":"10.1016/j.ijpt.2025.100740","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Robustness evaluation is critical for proton beam therapy (PBT) planning, but ideal robustness criteria are not clearly defined. Here, we compared robustness of PBT plans to published intensity-modulated radiation therapy (IMRT)-derived clinical target volume (CTV) robustness benchmarks and assessed the dosimetric impact of meeting IMRT-derived benchmarks on adjacent organs at risk.</p><p><strong>Patients and methods: </strong>Patients receiving PBT to 70 GyE in 28 fractions to the prostate alone from 2021 to 2022 at our institution were evaluated. PBT plan robustness was evaluated in nominal and worst-case data scenarios for CTV V100%, CTV V95%, rectum V70 Gy, and bladder V60 Gy. Clinically delivered (\"Clinical\") plans were compared to IMRT-derived worst-case CTV benchmarks. If benchmarks were not met, PBT plans were modified to meet both CTV V100% and V95% goals (\"Benchmark\" plans). Dosimetric comparisons between Clinical and Benchmark plans used a Wilcoxon signed-rank test with alpha set at 0.05.</p><p><strong>Results: </strong>Among 32 patients, median age and PSA at diagnosis were 71 years and 6.84 ng/mL, respectively. Most patients had favorable-intermediate risk disease (56.3%). Only 31% of clinical PBT met both worst-case CTV V100% > 90% and CTV V95% > 99% IMRT benchmarks. Plan renormalization (16 patients) or reoptimization (6 patients) resulted in all Benchmark plans meeting worst-case CTV thresholds. For Benchmark plans, nominal rectum V70 Gy increased from 0.72 to 0.92 cm<sup>3</sup>, and nominal bladder V60 Gy increased from 5.9% to 6.0% (<i>P</i> < .05 for each). Overall plan hot spot between Clinical and Benchmark plans increased from 104.5 to 105.5% (<i>P</i> < .05).</p><p><strong>Conclusion: </strong>When compared to an IMRT-derived benchmark for robustness coverage, Clinical PBT plans were less robust. However, all PBT plans were successfully modified to meet worst-case CTV benchmark with limited clinically expected impact on organ at risk dosimetry. Consideration should be made to adopt these benchmark criteria for prostate PBT.</p>","PeriodicalId":36923,"journal":{"name":"International Journal of Particle Therapy","volume":"15 ","pages":"100740"},"PeriodicalIF":2.0000,"publicationDate":"2025-02-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11889357/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Particle Therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1016/j.ijpt.2025.100740","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Robustness evaluation is critical for proton beam therapy (PBT) planning, but ideal robustness criteria are not clearly defined. Here, we compared robustness of PBT plans to published intensity-modulated radiation therapy (IMRT)-derived clinical target volume (CTV) robustness benchmarks and assessed the dosimetric impact of meeting IMRT-derived benchmarks on adjacent organs at risk.
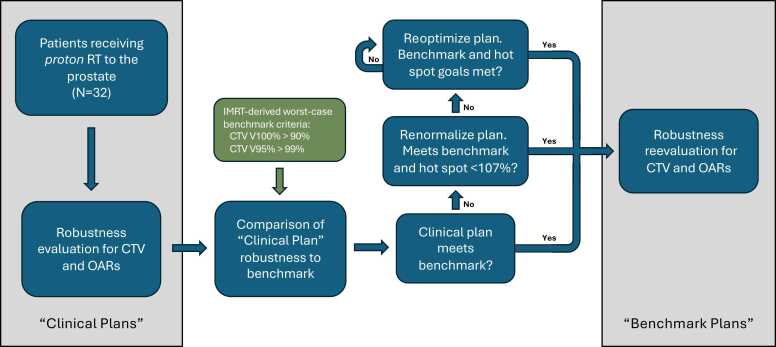
Patients and methods: Patients receiving PBT to 70 GyE in 28 fractions to the prostate alone from 2021 to 2022 at our institution were evaluated. PBT plan robustness was evaluated in nominal and worst-case data scenarios for CTV V100%, CTV V95%, rectum V70 Gy, and bladder V60 Gy. Clinically delivered ("Clinical") plans were compared to IMRT-derived worst-case CTV benchmarks. If benchmarks were not met, PBT plans were modified to meet both CTV V100% and V95% goals ("Benchmark" plans). Dosimetric comparisons between Clinical and Benchmark plans used a Wilcoxon signed-rank test with alpha set at 0.05.
Results: Among 32 patients, median age and PSA at diagnosis were 71 years and 6.84 ng/mL, respectively. Most patients had favorable-intermediate risk disease (56.3%). Only 31% of clinical PBT met both worst-case CTV V100% > 90% and CTV V95% > 99% IMRT benchmarks. Plan renormalization (16 patients) or reoptimization (6 patients) resulted in all Benchmark plans meeting worst-case CTV thresholds. For Benchmark plans, nominal rectum V70 Gy increased from 0.72 to 0.92 cm3, and nominal bladder V60 Gy increased from 5.9% to 6.0% (P < .05 for each). Overall plan hot spot between Clinical and Benchmark plans increased from 104.5 to 105.5% (P < .05).
Conclusion: When compared to an IMRT-derived benchmark for robustness coverage, Clinical PBT plans were less robust. However, all PBT plans were successfully modified to meet worst-case CTV benchmark with limited clinically expected impact on organ at risk dosimetry. Consideration should be made to adopt these benchmark criteria for prostate PBT.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


