Saumitra Rawat, Shyam Aggarwal, Purvish M Parikh, Adarsh Chaudhary, Manish Kumar, Mohit Sharma, Peush Sahni, Ramesh Ardhanari, R Pradeep, Amitabh Yadav, Suviraj John, C R Selvasekar
{"title":"Complete Mesocolic Excision for Colon Cancer: The New Standard of Care?","authors":"Saumitra Rawat, Shyam Aggarwal, Purvish M Parikh, Adarsh Chaudhary, Manish Kumar, Mohit Sharma, Peush Sahni, Ramesh Ardhanari, R Pradeep, Amitabh Yadav, Suviraj John, C R Selvasekar","doi":"10.1055/s-0044-1801754","DOIUrl":null,"url":null,"abstract":"<p><p>Complete mesocolic excision (CME) for colorectal cancer builds on the success of total mesorectal excision (TME), the international gold standard for rectal cancer. In TME, removal of the primary tumor along with associated mesocolon and accompanying structures as single intact specimen allows in toto excision of all structures that could potentially lead to dissemination. Recent meta-analysis has confirmed that CME results in better disease-free survival (DFS) and overall survival (OS) rates. CME can be done in three ways-open, laparoscopic, and robotic-assisted. We conducted a survey to identify the real-world situation with the use of CME by surgical oncologists. A total of 116 responders shared their experiences and thoughts. The benefit of CME was primarily thought to be for both OS and DFS by 78/116 (67%). The majority of CMEs are being conducted by the open method (74/116; 64%). A total of 52/116 (45%) were of the opinion that 6 to 10 surgeries constitute the learning curve for new surgeons for this technique. Based on our survey results, as well as two recently published systematic reviews and meta-analysis, it is time to consider CME as one of the standards of care in colorectal surgery.</p>","PeriodicalId":22053,"journal":{"name":"South Asian Journal of Cancer","volume":"13 4","pages":"251-258"},"PeriodicalIF":0.8000,"publicationDate":"2025-01-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11888812/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"South Asian Journal of Cancer","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0044-1801754","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
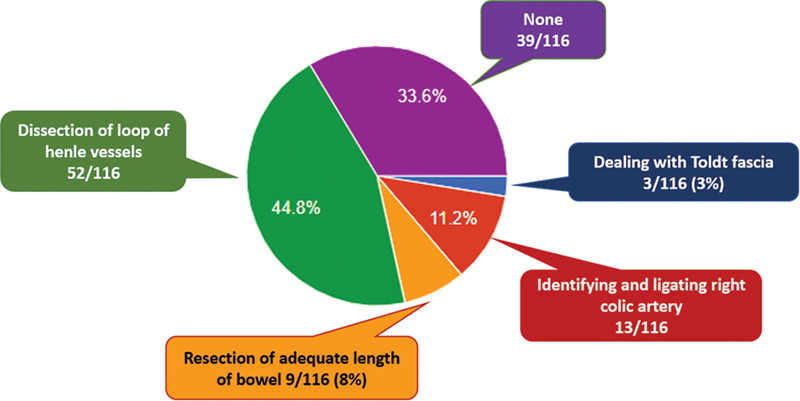
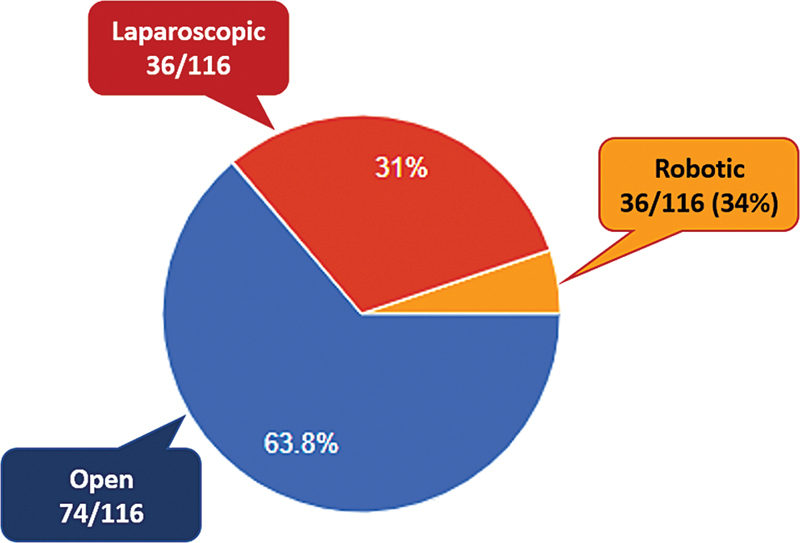
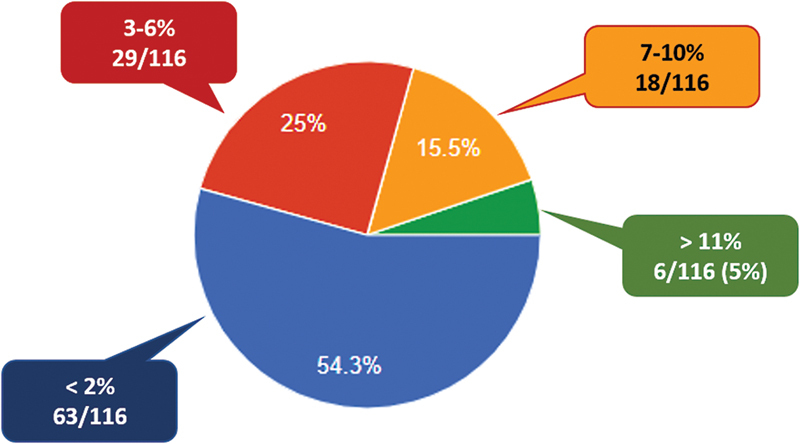
Complete mesocolic excision (CME) for colorectal cancer builds on the success of total mesorectal excision (TME), the international gold standard for rectal cancer. In TME, removal of the primary tumor along with associated mesocolon and accompanying structures as single intact specimen allows in toto excision of all structures that could potentially lead to dissemination. Recent meta-analysis has confirmed that CME results in better disease-free survival (DFS) and overall survival (OS) rates. CME can be done in three ways-open, laparoscopic, and robotic-assisted. We conducted a survey to identify the real-world situation with the use of CME by surgical oncologists. A total of 116 responders shared their experiences and thoughts. The benefit of CME was primarily thought to be for both OS and DFS by 78/116 (67%). The majority of CMEs are being conducted by the open method (74/116; 64%). A total of 52/116 (45%) were of the opinion that 6 to 10 surgeries constitute the learning curve for new surgeons for this technique. Based on our survey results, as well as two recently published systematic reviews and meta-analysis, it is time to consider CME as one of the standards of care in colorectal surgery.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


