Burhan Dost, Hilal Hanife Kandemir, Kubra Tabur, Sule Nur Karakurt, Beliz Yayla, Canan Asar Sahin, Cengiz Kaya
{"title":"Intrathecal morphine vs. Ultrasound-guided bilateral posterior quadratus lumborum block in caesarean delivery.","authors":"Burhan Dost, Hilal Hanife Kandemir, Kubra Tabur, Sule Nur Karakurt, Beliz Yayla, Canan Asar Sahin, Cengiz Kaya","doi":"10.1186/s44158-025-00235-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Effective postoperative pain management is crucial in caesarean delivery (CD) to enhance recovery, minimize opioid use, and improve maternal outcomes. Intrathecal morphine (ITM) is widely used but can cause side effects, such as pruritus and nausea. Posterior quadratus lumborum block (QLB) has emerged as a potential alternative for postoperative analgesia. This study compared the analgesic efficacy and side-effect profiles of ITM and posterior QLB in patients with CD.</p><p><strong>Methods: </strong>This prospective observational study included parturients who underwent elective CD under spinal anesthesia. Participants were allocated to receive either ITM (100 µg) or bilateral posterior QLB with 0.25% bupivacaine (25 mL per side). The primary outcome was cumulative intravenous morphine consumption 24 h post-surgery. The secondary outcomes included NRS pain scores at rest and during activity at 0, 3, 6, 12, and 24 h, the time to first opioid request, the number of patients requiring rescue analgesia, nausea and vomiting scores, pruritus scores, and scores on the Obstetric Quality of Recovery Scale (ObsQoR-11 T) at 24 h and 48 h postoperatively.</p><p><strong>Results: </strong>Sixty patients were included in the analysis, with 30 patients in each group. The primary outcome, 24-h cumulative intravenous morphine consumption, was comparable between the ITM and posterior QLB groups (6 [10] mg vs. 8.2 [7.1] mg, p = 0.134). The secondary outcomes, including NRS pain scores at rest and during activity, time to first opioid request, number of patients requiring rescue analgesia (1 vs. 0; p = 0.313), nausea and vomiting scores, pruritus scores (0 [1] vs. 0 [0]; p = 0.234), and ObsQoR-11 T scores at 24 h (95.5 [14] vs. 87.5 [16]; p = 0.49) and 48 h (102 [13] vs. 97 [18]; p = 0.203), were not significantly different between the groups.</p><p><strong>Conclusion: </strong>Both ITM and posterior QLB provide effective postoperative analgesia in patients with CD, with comparable analgesic outcomes and side-effect profiles. ITM remains a practical choice because of its ease of administration, whereas subsequent QLB serves as a viable alternative for patients intolerant to neuraxial opioids.</p>","PeriodicalId":73597,"journal":{"name":"Journal of Anesthesia, Analgesia and Critical Care (Online)","volume":"5 1","pages":"14"},"PeriodicalIF":3.1000,"publicationDate":"2025-03-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11887214/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Anesthesia, Analgesia and Critical Care (Online)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s44158-025-00235-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Effective postoperative pain management is crucial in caesarean delivery (CD) to enhance recovery, minimize opioid use, and improve maternal outcomes. Intrathecal morphine (ITM) is widely used but can cause side effects, such as pruritus and nausea. Posterior quadratus lumborum block (QLB) has emerged as a potential alternative for postoperative analgesia. This study compared the analgesic efficacy and side-effect profiles of ITM and posterior QLB in patients with CD.
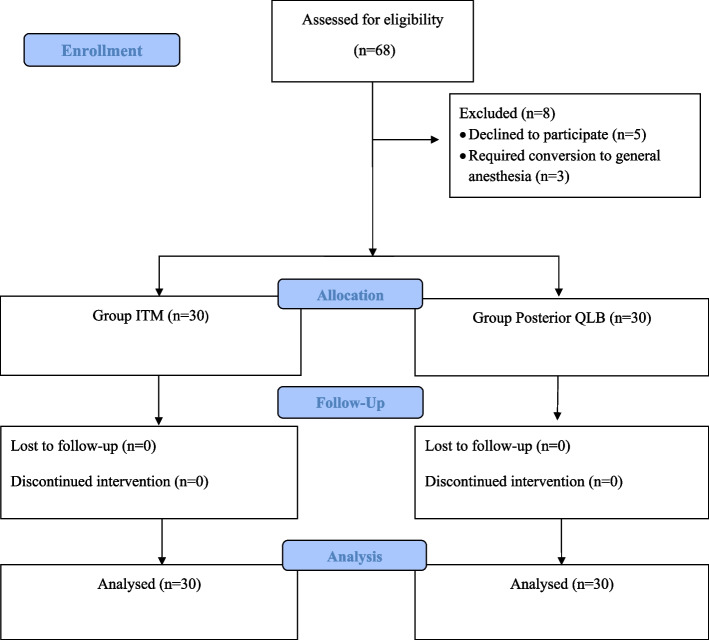
Methods: This prospective observational study included parturients who underwent elective CD under spinal anesthesia. Participants were allocated to receive either ITM (100 µg) or bilateral posterior QLB with 0.25% bupivacaine (25 mL per side). The primary outcome was cumulative intravenous morphine consumption 24 h post-surgery. The secondary outcomes included NRS pain scores at rest and during activity at 0, 3, 6, 12, and 24 h, the time to first opioid request, the number of patients requiring rescue analgesia, nausea and vomiting scores, pruritus scores, and scores on the Obstetric Quality of Recovery Scale (ObsQoR-11 T) at 24 h and 48 h postoperatively.
Results: Sixty patients were included in the analysis, with 30 patients in each group. The primary outcome, 24-h cumulative intravenous morphine consumption, was comparable between the ITM and posterior QLB groups (6 [10] mg vs. 8.2 [7.1] mg, p = 0.134). The secondary outcomes, including NRS pain scores at rest and during activity, time to first opioid request, number of patients requiring rescue analgesia (1 vs. 0; p = 0.313), nausea and vomiting scores, pruritus scores (0 [1] vs. 0 [0]; p = 0.234), and ObsQoR-11 T scores at 24 h (95.5 [14] vs. 87.5 [16]; p = 0.49) and 48 h (102 [13] vs. 97 [18]; p = 0.203), were not significantly different between the groups.
Conclusion: Both ITM and posterior QLB provide effective postoperative analgesia in patients with CD, with comparable analgesic outcomes and side-effect profiles. ITM remains a practical choice because of its ease of administration, whereas subsequent QLB serves as a viable alternative for patients intolerant to neuraxial opioids.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


