Gorka Barrenetxea, Olaia Prego, Ricardo Celis, Edurne Martínez, María De Las Heras, Oihane Gómez, Olaia Aguirre, Sheila Samojluk, Julen Barrenetxea
{"title":"Effects of vaginal vs oral progesterone supplementation before embryo transfer on live birth rates and levels: a randomized trial.","authors":"Gorka Barrenetxea, Olaia Prego, Ricardo Celis, Edurne Martínez, María De Las Heras, Oihane Gómez, Olaia Aguirre, Sheila Samojluk, Julen Barrenetxea","doi":"10.1530/RAF-24-0094","DOIUrl":null,"url":null,"abstract":"<p><strong>Abstract: </strong>The increase in frozen embryo transfers (FETs) is a consequence of advances in embryo vitrification and the implementation of genetic screening of embryos. There is debate over the best progesterone administration route in substituted cycles and the relationship between progesterone levels on embryo transfer (ET) day and reproductive outcomes. This trial aimed to compare the clinical results of different progesterone supplementation schedules before ET and assess the relationship between plasmatic progesterone levels on transfer day and clinical outcomes. In a prospective, randomized, controlled study, 500 patients were randomly divided into two groups based on the progesterone administration route (oral or vaginal) before ET. Progesterone levels were measured on ET day (PP1) and B-HCG determination (PP2). The primary endpoint was the live birth rate according to different progesterone schedules and levels on transfer day. Despite higher plasmatic progesterone levels with oral administration compared to the vaginal route, there were no significant differences in clinical pregnancy (50.20 vs 47.37%), live birth (43.67 vs 40.89%) or miscarriage rates (13.01 vs 13.68%). Progesterone levels on transfer day were significantly higher among ongoing pregnancies (24.96 ± 1.00 ng/mL) compared to non-ongoing pregnancies (19.39 ± 1.47 ng/mL) and non-pregnancies (17.56 ± 0.99 ng/mL) (P = 0.0001).</p><p><strong>Lay summary: </strong>The use of FET for the treatment of infertility is increasing. There are two key ongoing debates. First, consensus still needs to be reached regarding the most effective method for preparing the endometrial lining regarding maternal and neonatal outcomes. Second, the optimal progesterone level on the day of ET remains unclear. While how progesterone is administered affects its concentration, no significant differences in clinical outcomes have been observed. However, successful pregnancies tend to have higher progesterone levels than others. Given that the way progesterone is administered does not affect pregnancy rates, patient preferences should guide protocol choices, and further research is needed to explore the association between low progesterone levels on the day of ET and poorer reproductive outcomes.</p><p><strong>Trial registration number: </strong>EUDRACT: 2022-000382-41. The clinical trial was approved by the AEMPS (Agencia Española de Productos Sanitarios y Medicamentos; Spanish Agency for Medicines and Health Products) and the local Drugs Research Ethics Committee (CEIm-E). The Institutional Review Board approved the trial.</p><p><strong>Trial registration date: </strong>24 August 2022. Date of first patient's enrolment: 10 September 2022.</p>","PeriodicalId":101312,"journal":{"name":"Reproduction & fertility","volume":" ","pages":""},"PeriodicalIF":3.4000,"publicationDate":"2025-03-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11949523/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Reproduction & fertility","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1530/RAF-24-0094","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"Print","JCR":"Q2","JCRName":"REPRODUCTIVE BIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
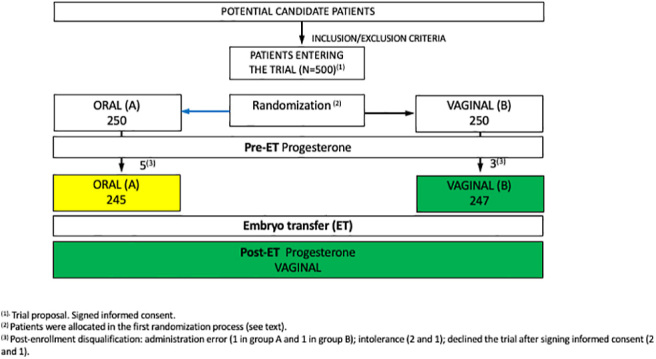
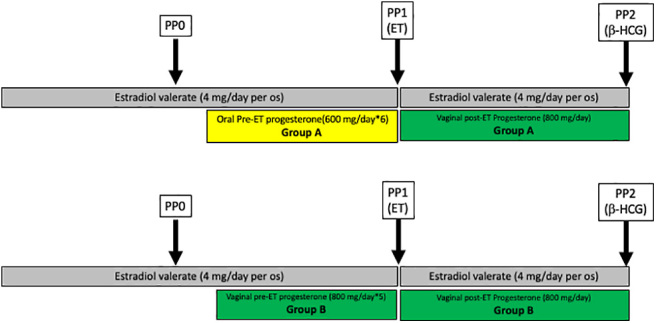
Abstract: The increase in frozen embryo transfers (FETs) is a consequence of advances in embryo vitrification and the implementation of genetic screening of embryos. There is debate over the best progesterone administration route in substituted cycles and the relationship between progesterone levels on embryo transfer (ET) day and reproductive outcomes. This trial aimed to compare the clinical results of different progesterone supplementation schedules before ET and assess the relationship between plasmatic progesterone levels on transfer day and clinical outcomes. In a prospective, randomized, controlled study, 500 patients were randomly divided into two groups based on the progesterone administration route (oral or vaginal) before ET. Progesterone levels were measured on ET day (PP1) and B-HCG determination (PP2). The primary endpoint was the live birth rate according to different progesterone schedules and levels on transfer day. Despite higher plasmatic progesterone levels with oral administration compared to the vaginal route, there were no significant differences in clinical pregnancy (50.20 vs 47.37%), live birth (43.67 vs 40.89%) or miscarriage rates (13.01 vs 13.68%). Progesterone levels on transfer day were significantly higher among ongoing pregnancies (24.96 ± 1.00 ng/mL) compared to non-ongoing pregnancies (19.39 ± 1.47 ng/mL) and non-pregnancies (17.56 ± 0.99 ng/mL) (P = 0.0001).
Lay summary: The use of FET for the treatment of infertility is increasing. There are two key ongoing debates. First, consensus still needs to be reached regarding the most effective method for preparing the endometrial lining regarding maternal and neonatal outcomes. Second, the optimal progesterone level on the day of ET remains unclear. While how progesterone is administered affects its concentration, no significant differences in clinical outcomes have been observed. However, successful pregnancies tend to have higher progesterone levels than others. Given that the way progesterone is administered does not affect pregnancy rates, patient preferences should guide protocol choices, and further research is needed to explore the association between low progesterone levels on the day of ET and poorer reproductive outcomes.
Trial registration number: EUDRACT: 2022-000382-41. The clinical trial was approved by the AEMPS (Agencia Española de Productos Sanitarios y Medicamentos; Spanish Agency for Medicines and Health Products) and the local Drugs Research Ethics Committee (CEIm-E). The Institutional Review Board approved the trial.
Trial registration date: 24 August 2022. Date of first patient's enrolment: 10 September 2022.
冷冻胚胎移植的增加是胚胎玻璃化和胚胎遗传筛选技术进步的结果。关于替代周期中黄体酮的最佳给药途径以及胚胎移植日黄体酮水平与生殖结局的关系存在争议。本试验旨在比较胚胎移植前不同黄体酮补充计划的临床结果,并评估移植当日血浆黄体酮水平与临床结果的关系。在一项前瞻性、随机、对照研究中,500名患者根据胚胎移植前黄体酮给药途径(口服或阴道)随机分为两组。测定胚胎移植日黄体酮水平(PP1)和B-HCG水平(PP2)。主要终点是根据不同的黄体酮方案和移植当天黄体酮水平的活产率。尽管口服给药与阴道给药相比血浆黄体酮水平较高,但在临床妊娠(50.20% vs. 47.37%)、活产(43.67% vs. 40.89%)或流产率(13.33% vs. 6.48%)方面没有显著差异。妊娠患者移植当日孕酮水平(24.96±1.00 ng/ml)显著高于未妊娠患者(18.02±1.07 ng/ml) (p=0.001)。在妊娠试验阳性的患者中,进展性妊娠和非进展性妊娠之间的差异无统计学意义。总之,虽然不同的黄体酮给药途径导致胚胎移植(ET)当天的血浆水平不同,但这些差异并不影响生殖结果。


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


