{"title":"Prevalence and predictability of the Chicago Classification of Pouchitis in ulcerative colitis: a multicenter study in Japan.","authors":"Shintaro Akiyama, Ryohei Hayashi, Takeshi Takasago, Kurando Kusunoki, Hiroki Ikeuchi, Kento Takenaka, Kazuhiro Watanabe, Kazutaka Koganei, Nobuhiro Ueno, Mikihiro Fujiya, Naoki Hosoe, Fumikazu Koyama, Yasuhisa Sakata, Motohiro Esaki, Ken Takeuchi, Makoto Naganuma, Kiichiro Tsuchiya","doi":"10.1007/s00535-025-02231-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Endoscopic phenotypes of pouchitis according to the Chicago Classification have been reported to be associated with poor pouch outcomes in ulcerative colitis (UC). Here, we aimed to assess the prevalence of endoscopic phenotypes and their predictability for pouch outcomes.</p><p><strong>Methods: </strong>This retrospective multicenter study included UC patients aged 18 years or older who underwent total colectomy between January 2000 and March 2020. The primary endpoints were frequencies of endoscopic phenotypes of the Chicago Classification and their predictability for chronic pouchitis and pouch failure. Endoscopic findings were evaluated at the initial pouchoscopy and at 3 and 10 years after ileostomy takedown.</p><p><strong>Results: </strong>A total of 392 eligible patients were identified. The frequencies of chronic pouchitis and pouch failure were 32% and 4.9%, respectively. Focal inflammation and inlet involvement at the initial postoperative pouchoscopy were significantly associated with subsequent risk of chronic pouchitis and pouch failure, respectively. Thirty percent of the patients with focal inflammation progressed to diffuse inflammation when chronic pouchitis developed. Multivariate analysis showed chronic pouchitis was significantly associated with diffuse inflammation and cuffitis observed throughout the clinical course. The proportion of pouch-related fistula was significantly lower in our cohort than in the US cohort (4.8% vs 19%, P < 0.001), and pouch-related fistula was an independent risk factor for pouch failure.</p><p><strong>Conclusions: </strong>We demonstrated the predictability of the Chicago Classification for pouch outcomes, and a lower prevalence of pouch-related fistula, resulting in a lower pouch failure risk in our multicenter cohort.</p>","PeriodicalId":16059,"journal":{"name":"Journal of Gastroenterology","volume":" ","pages":"715-726"},"PeriodicalIF":5.5000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12095421/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Gastroenterology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00535-025-02231-1","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/6 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Endoscopic phenotypes of pouchitis according to the Chicago Classification have been reported to be associated with poor pouch outcomes in ulcerative colitis (UC). Here, we aimed to assess the prevalence of endoscopic phenotypes and their predictability for pouch outcomes.
Methods: This retrospective multicenter study included UC patients aged 18 years or older who underwent total colectomy between January 2000 and March 2020. The primary endpoints were frequencies of endoscopic phenotypes of the Chicago Classification and their predictability for chronic pouchitis and pouch failure. Endoscopic findings were evaluated at the initial pouchoscopy and at 3 and 10 years after ileostomy takedown.
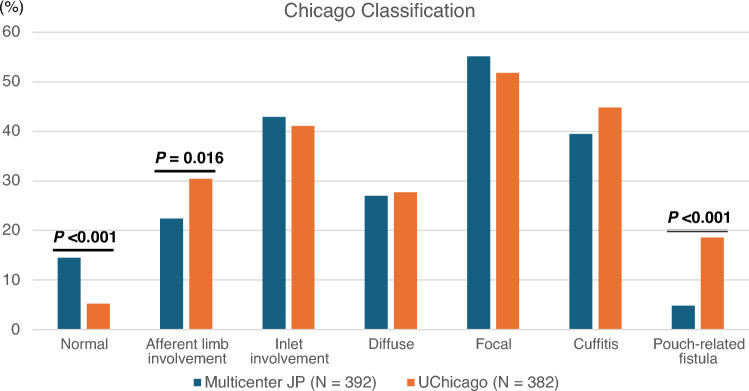
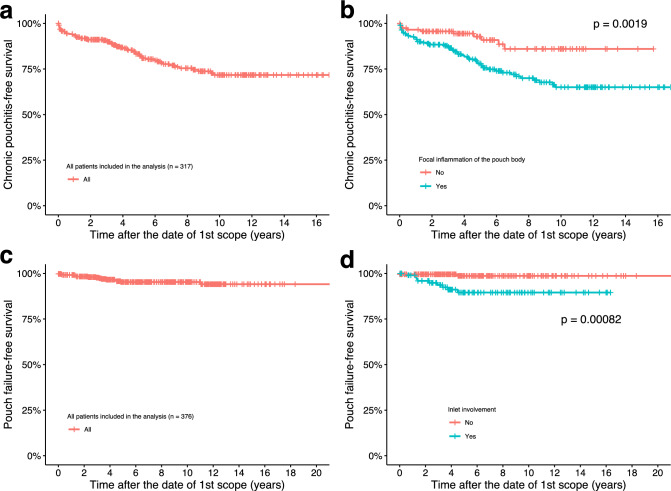
Results: A total of 392 eligible patients were identified. The frequencies of chronic pouchitis and pouch failure were 32% and 4.9%, respectively. Focal inflammation and inlet involvement at the initial postoperative pouchoscopy were significantly associated with subsequent risk of chronic pouchitis and pouch failure, respectively. Thirty percent of the patients with focal inflammation progressed to diffuse inflammation when chronic pouchitis developed. Multivariate analysis showed chronic pouchitis was significantly associated with diffuse inflammation and cuffitis observed throughout the clinical course. The proportion of pouch-related fistula was significantly lower in our cohort than in the US cohort (4.8% vs 19%, P < 0.001), and pouch-related fistula was an independent risk factor for pouch failure.
Conclusions: We demonstrated the predictability of the Chicago Classification for pouch outcomes, and a lower prevalence of pouch-related fistula, resulting in a lower pouch failure risk in our multicenter cohort.
背景:据报道,根据芝加哥分类法,眼袋炎的内镜表型与溃疡性结肠炎(UC)的眼袋预后不良有关。在这里,我们的目的是评估内窥镜表型的患病率及其对眼袋结局的可预测性。方法:这项回顾性多中心研究纳入了2000年1月至2020年3月期间接受全结肠切除术的18岁或以上的UC患者。主要终点是芝加哥分类的内窥镜表型频率及其对慢性眼袋炎和眼袋衰竭的可预测性。内窥镜检查结果在最初的袋镜检查和回肠造口术后3年和10年进行评估。结果:共确定392例符合条件的患者。慢性眼袋炎和眼袋衰竭的发生率分别为32%和4.9%。术后初始袋镜检查时的局灶性炎症和进气道受累性分别与随后发生慢性袋炎和袋衰竭的风险显著相关。慢性袋炎发生时,30%的局灶性炎症发展为弥漫性炎症。多变量分析显示慢性袋炎与弥漫性炎症和袖炎在整个临床过程中观察到显著相关。在我们的队列中,眼袋相关瘘管的比例明显低于美国队列(4.8% vs 19%)。结论:我们证明了芝加哥分类对眼袋结局的可预测性,以及较低的眼袋相关瘘管患病率,从而在我们的多中心队列中降低了眼袋失败的风险。
期刊介绍:
The Journal of Gastroenterology, which is the official publication of the Japanese Society of Gastroenterology, publishes Original Articles (Alimentary Tract/Liver, Pancreas, and Biliary Tract), Review Articles, Letters to the Editors and other articles on all aspects of the field of gastroenterology. Significant contributions relating to basic research, theory, and practice are welcomed. These publications are designed to disseminate knowledge in this field to a worldwide audience, and accordingly, its editorial board has an international membership.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


