Edmund Wedam Kanmiki, Abdullah A Mamun, James F Phillips, Martin O'Flaherty
{"title":"Equity effect of a community-based primary healthcare program on the incidence of childhood morbidity in rural Northern Ghana.","authors":"Edmund Wedam Kanmiki, Abdullah A Mamun, James F Phillips, Martin O'Flaherty","doi":"10.1017/S1463423625000106","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Childhood morbidity is a precursor and contributor to under-five child mortality. Community-based primary healthcare programs are culturally responsive and low-cost strategies for delivering maternal and child health services in rural communities.</p><p><strong>Aim: </strong>To evaluate the equity effect of the Ghana Essential Health Intervention Program (GEHIP) - a five-year community-based primary healthcare program - on childhood morbidity.</p><p><strong>Methods: </strong>GEHIP was implemented in the Upper East region of Northern Ghana. Household baseline and end line surveys conducted in 2010/2011 and 2014/2015, respectively, from both intervention and comparison districts were used to assess three childhood morbidity conditions: maternal recall of neonatal illness, the incidence of diarrhoea, and fever. Difference-in-differences analysis, mean comparison test, and multivariate logistic regressions are used to assess the effect of GEHIP exposure on these three childhood morbidity conditions.</p><p><strong>Results: </strong>Baseline sample data of 2,911 women and end line sample of 2,829 women were included in this analysis. There was generally more reduction in all three childhood morbidity conditions in intervention communities relative to comparison communities. Diarrhoea and fever had a statistically significant treatment effect (AOR = 0.95, p-value<0.01 and AOR = 0.94, p-value<0.001). Results of equity analysis indicate significant mean reductions for both the poor and non-poor for neonatal illness and diarrhea, while only the intervention group had a significant reduction for both poor and non-poor for fever. Regression analysis shows no significant equity/inequity effects of GEHIP on the incidence of diarrhoea and fever. Neonatal illness, however, shows significant effects of wealth within the intervention group.</p><p><strong>Conclusion: </strong>This study shows that GEHIP contributed significantly to childhood morbidity reduction. This implies that community-based strategies have the potential to improve child health and contribute to the attainment of the United Nations sustainable development goal related to child health. Specific targeted measures are recommended to ensure both the poor and relatively better-off benefit from interventions.</p>","PeriodicalId":74493,"journal":{"name":"Primary health care research & development","volume":"26 ","pages":"e23"},"PeriodicalIF":1.7000,"publicationDate":"2025-02-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11883786/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Primary health care research & development","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1017/S1463423625000106","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Childhood morbidity is a precursor and contributor to under-five child mortality. Community-based primary healthcare programs are culturally responsive and low-cost strategies for delivering maternal and child health services in rural communities.
Aim: To evaluate the equity effect of the Ghana Essential Health Intervention Program (GEHIP) - a five-year community-based primary healthcare program - on childhood morbidity.
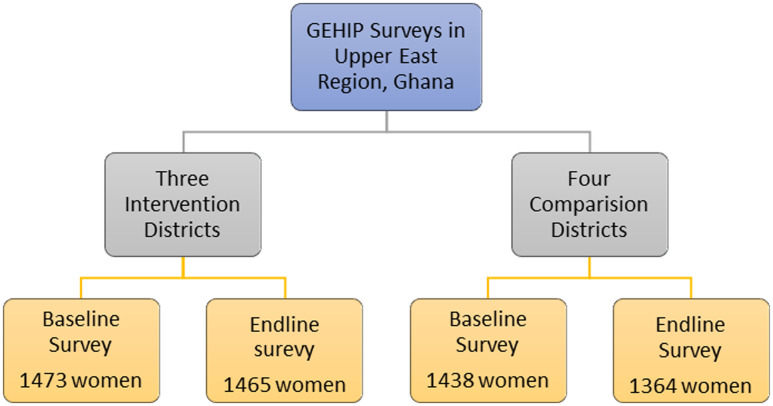
Methods: GEHIP was implemented in the Upper East region of Northern Ghana. Household baseline and end line surveys conducted in 2010/2011 and 2014/2015, respectively, from both intervention and comparison districts were used to assess three childhood morbidity conditions: maternal recall of neonatal illness, the incidence of diarrhoea, and fever. Difference-in-differences analysis, mean comparison test, and multivariate logistic regressions are used to assess the effect of GEHIP exposure on these three childhood morbidity conditions.
Results: Baseline sample data of 2,911 women and end line sample of 2,829 women were included in this analysis. There was generally more reduction in all three childhood morbidity conditions in intervention communities relative to comparison communities. Diarrhoea and fever had a statistically significant treatment effect (AOR = 0.95, p-value<0.01 and AOR = 0.94, p-value<0.001). Results of equity analysis indicate significant mean reductions for both the poor and non-poor for neonatal illness and diarrhea, while only the intervention group had a significant reduction for both poor and non-poor for fever. Regression analysis shows no significant equity/inequity effects of GEHIP on the incidence of diarrhoea and fever. Neonatal illness, however, shows significant effects of wealth within the intervention group.
Conclusion: This study shows that GEHIP contributed significantly to childhood morbidity reduction. This implies that community-based strategies have the potential to improve child health and contribute to the attainment of the United Nations sustainable development goal related to child health. Specific targeted measures are recommended to ensure both the poor and relatively better-off benefit from interventions.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


