Correlation between a real-time bioparticle detection device and a traditional microbiological active air sampler monitoring air quality in an operating room during elective arthroplasty surgery: a prospective feasibility study.
Lise-Lott Larsson, Johan Nordenadler, Gunilla Björling, Li Felländer-Tsai, Stergios Lazarinis, Bengt Ljungqvist, Janet Mattsson, Berit Reinmüller, Harald Brismar
{"title":"Correlation between a real-time bioparticle detection device and a traditional microbiological active air sampler monitoring air quality in an operating room during elective arthroplasty surgery: a prospective feasibility study.","authors":"Lise-Lott Larsson, Johan Nordenadler, Gunilla Björling, Li Felländer-Tsai, Stergios Lazarinis, Bengt Ljungqvist, Janet Mattsson, Berit Reinmüller, Harald Brismar","doi":"10.2340/17453674.2025.43002","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and purpose: </strong>The standard method for controlling operating room (OR) air quality is measuring bacteria-carrying particles per volume unit of air: colony forming units (CFU/m3). The result takes at least 2 days after sampling. Another method is real-time measurements of fluorescing bioparticles per unit volume of air (FBP/dm3). We aimed to compare simultaneous measurements of FBP/50 dm3 and CFU/m3 during ongoing arthroplasty surgery.</p><p><strong>Methods: </strong>18 arthroplasties were performed in a modern OR with turbulent mixed airflow ventilation. The sampling heads of a BioAerosol Monitoring System (BAMS) and a microbiological active air sampler (Sartorius MD8 Air Sampler) were placed next to each other, and 6 parallel 10-minute registrations of FBP/50 dm3 and CFU/m3 were performed for each surgery. Parallel measurements were plotted against each other, Passing-Bablok nonparametric linear regression was performed, and the Spearman correlation coefficient (r) was calculated.</p><p><strong>Results: </strong>The r between FBP ≥ 3 μm/50 dm3 and CFU/m3 sampled for 96 x 10-minute intervals, was 0.70 (95% confidence interval [CI] 0.57-0.79). In the 25th percentile with the lowest 10-minute FBP ≥ 3μm/50 dm3, there were no CFU measurements with ≥ 10 and 4% with ≥ 5 CFU/m3. In the 75th percentile with the highest 10-minute FBP ≥ 3 μm/50 dm3, there were 58% CFU measurements with ≥ 10 and 88% with ≥ 5 CFU/m3. The r between FBP ≥ 3 μm/50 dm3 and CFU/m3 means sampled during 18 operations was 0.87 (CI 0.68-0.95).</p><p><strong>Conclusion: </strong>Low FBP ≥ 3 μm/50 dm3 measured by BAMS indicates low CFU/m3; conversely, high FBP ≥ 3 μm/50 dm3 indicates high CFU/m3. Real-time measurements of FBP ≥ 3 μm/50 dm3 can be used as a supplement to CFU/m3 monitoring OR air bacterial load.</p>","PeriodicalId":6916,"journal":{"name":"Acta Orthopaedica","volume":"96 ","pages":"176-181"},"PeriodicalIF":2.4000,"publicationDate":"2025-02-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11849163/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta Orthopaedica","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2340/17453674.2025.43002","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background and purpose: The standard method for controlling operating room (OR) air quality is measuring bacteria-carrying particles per volume unit of air: colony forming units (CFU/m3). The result takes at least 2 days after sampling. Another method is real-time measurements of fluorescing bioparticles per unit volume of air (FBP/dm3). We aimed to compare simultaneous measurements of FBP/50 dm3 and CFU/m3 during ongoing arthroplasty surgery.
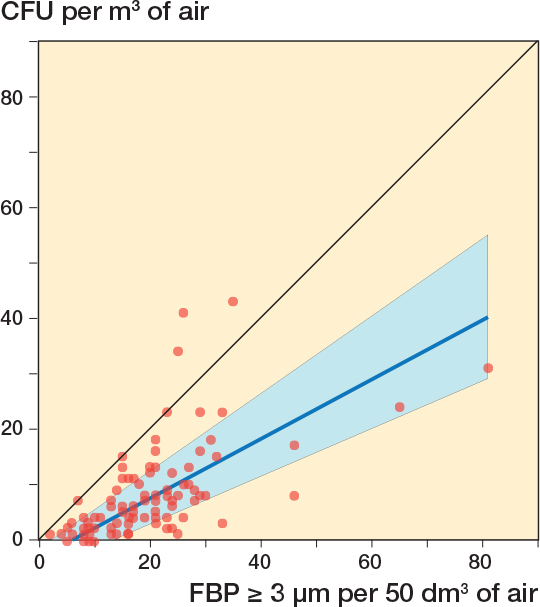
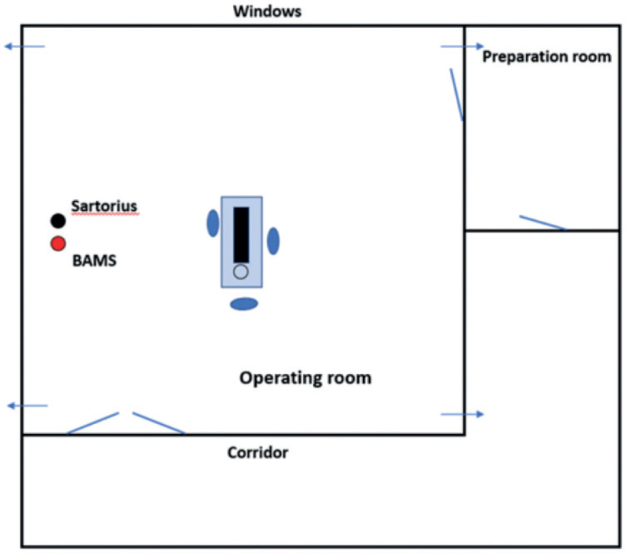
Methods: 18 arthroplasties were performed in a modern OR with turbulent mixed airflow ventilation. The sampling heads of a BioAerosol Monitoring System (BAMS) and a microbiological active air sampler (Sartorius MD8 Air Sampler) were placed next to each other, and 6 parallel 10-minute registrations of FBP/50 dm3 and CFU/m3 were performed for each surgery. Parallel measurements were plotted against each other, Passing-Bablok nonparametric linear regression was performed, and the Spearman correlation coefficient (r) was calculated.
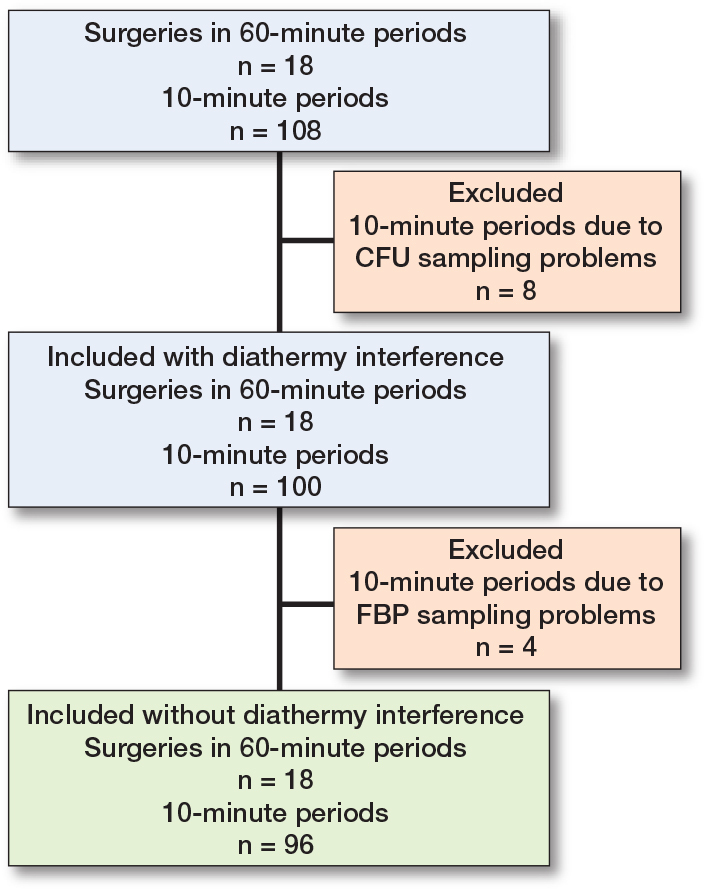
Results: The r between FBP ≥ 3 μm/50 dm3 and CFU/m3 sampled for 96 x 10-minute intervals, was 0.70 (95% confidence interval [CI] 0.57-0.79). In the 25th percentile with the lowest 10-minute FBP ≥ 3μm/50 dm3, there were no CFU measurements with ≥ 10 and 4% with ≥ 5 CFU/m3. In the 75th percentile with the highest 10-minute FBP ≥ 3 μm/50 dm3, there were 58% CFU measurements with ≥ 10 and 88% with ≥ 5 CFU/m3. The r between FBP ≥ 3 μm/50 dm3 and CFU/m3 means sampled during 18 operations was 0.87 (CI 0.68-0.95).
Conclusion: Low FBP ≥ 3 μm/50 dm3 measured by BAMS indicates low CFU/m3; conversely, high FBP ≥ 3 μm/50 dm3 indicates high CFU/m3. Real-time measurements of FBP ≥ 3 μm/50 dm3 can be used as a supplement to CFU/m3 monitoring OR air bacterial load.
期刊介绍:
Acta Orthopaedica (previously Acta Orthopaedica Scandinavica) presents original articles of basic research interest, as well as clinical studies in the field of orthopedics and related sub disciplines. Ever since the journal was founded in 1930, by a group of Scandinavian orthopedic surgeons, the journal has been published for an international audience. Acta Orthopaedica is owned by the Nordic Orthopaedic Federation and is the official publication of this federation.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


