Satisfaction and quality of dying with nonoperative end-of-life care for hospitalized and non-hospitalized frail older patients with (suspected) hip fractures: a combined cohort study.
Miliaan L Zeelenberg, Sverre A I Loggers, Pieter Joosse, Esther M M Van Lieshout, Taco Gosens
{"title":"Satisfaction and quality of dying with nonoperative end-of-life care for hospitalized and non-hospitalized frail older patients with (suspected) hip fractures: a combined cohort study.","authors":"Miliaan L Zeelenberg, Sverre A I Loggers, Pieter Joosse, Esther M M Van Lieshout, Taco Gosens","doi":"10.2340/17453674.2025.42998","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and purpose: </strong>For frail institutionalized hip fracture patients who opt for nonoperative management (NOM), the additional treatment benefits of hospital admission and in-hospital diagnostics are not well evaluated. We aimed to describe and compare treatment satisfaction and quality of dying for patients who refrained from hospitalization after a hip fracture and patients who were treated nonoperatively after a short period of hospitalization.</p><p><strong>Methods: </strong>Both cohorts included very frail institutionalized hip fracture patients. The first group directly started supportive care in their own nursing home after a suspected hip fracture. The second opted for NOM during shared decision-making after admission and diagnostics at the hospital. Primary outcomes were treatment satisfaction and quality of dying measured by the Quality of Dying and Death Questionnaire (QODD). Secondary outcomes included health-related quality of life (EuroQoL-5D-5L and Qualidem), pain, and medication.</p><p><strong>Results: </strong>20 non-hospitalized and 88 hospitalized patients were included. Overall treatment satisfaction by proxies was high for both the non-hospitalized 9 (interquartile range [IQR] 8-10) and hospitalized patients 8 (IQR 4-9). Quality of dying was rated higher in the non-hospitalized group with QODD 8.3, IQR 6.9-8.6 versus 7.0, IQR 5.7-7.8, and median difference 1.0 (95% confidence interval [CI] 0.1-1.8). Health-related quality of life, measured by the EQ-5D-5L utility score, was low in both groups but higher in non-hospitalized patients (0.30, IQR 0.15-0.32) than in hospitalized patients (0.25, IQR 0.03-0.32, median difference: 0.03, CI -0.03 to 0.09). Both groups reported similar pain levels, but hospitalized patients used higher standardized daily doses of opiates (68 mg vs 39 mg, median difference 24 mg, CI 7-42).</p><p><strong>Conclusion: </strong>Proxies of hospitalized and non-hospitalized patients report high treatment satisfaction after opting for NOM. Non-hospitalization may have a beneficial effect on quality of dying in selected patients who have pre-recorded do-not-hospitalize directives or shared decision-making after a suspected hip fracture.</p>","PeriodicalId":6916,"journal":{"name":"Acta Orthopaedica","volume":"96 ","pages":"167-173"},"PeriodicalIF":2.4000,"publicationDate":"2025-02-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11849162/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta Orthopaedica","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2340/17453674.2025.42998","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background and purpose: For frail institutionalized hip fracture patients who opt for nonoperative management (NOM), the additional treatment benefits of hospital admission and in-hospital diagnostics are not well evaluated. We aimed to describe and compare treatment satisfaction and quality of dying for patients who refrained from hospitalization after a hip fracture and patients who were treated nonoperatively after a short period of hospitalization.
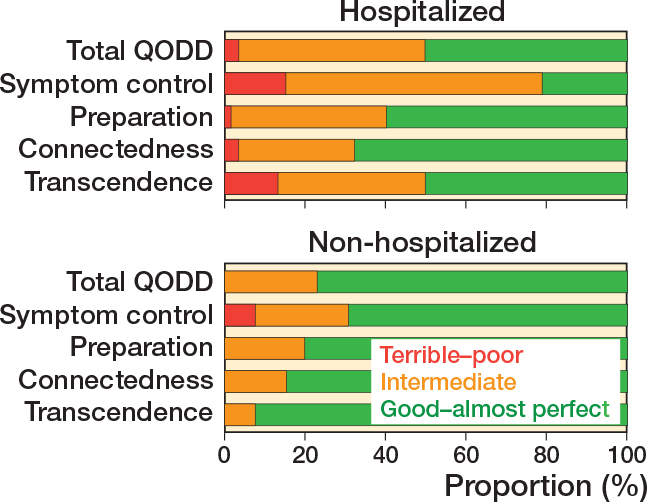
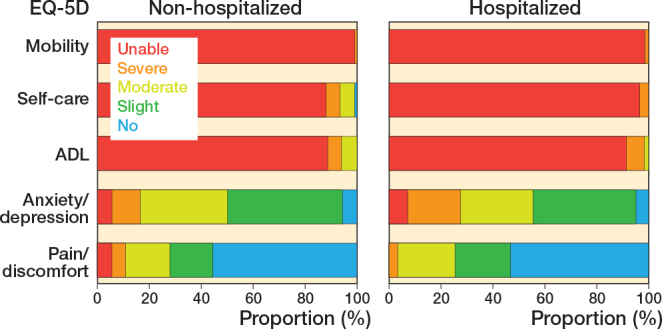
Methods: Both cohorts included very frail institutionalized hip fracture patients. The first group directly started supportive care in their own nursing home after a suspected hip fracture. The second opted for NOM during shared decision-making after admission and diagnostics at the hospital. Primary outcomes were treatment satisfaction and quality of dying measured by the Quality of Dying and Death Questionnaire (QODD). Secondary outcomes included health-related quality of life (EuroQoL-5D-5L and Qualidem), pain, and medication.
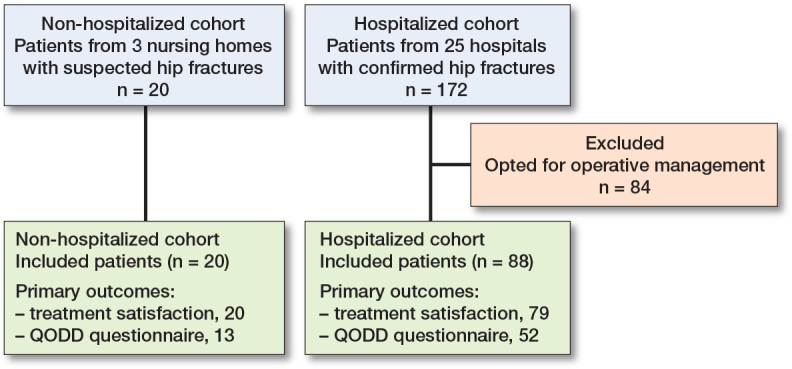
Results: 20 non-hospitalized and 88 hospitalized patients were included. Overall treatment satisfaction by proxies was high for both the non-hospitalized 9 (interquartile range [IQR] 8-10) and hospitalized patients 8 (IQR 4-9). Quality of dying was rated higher in the non-hospitalized group with QODD 8.3, IQR 6.9-8.6 versus 7.0, IQR 5.7-7.8, and median difference 1.0 (95% confidence interval [CI] 0.1-1.8). Health-related quality of life, measured by the EQ-5D-5L utility score, was low in both groups but higher in non-hospitalized patients (0.30, IQR 0.15-0.32) than in hospitalized patients (0.25, IQR 0.03-0.32, median difference: 0.03, CI -0.03 to 0.09). Both groups reported similar pain levels, but hospitalized patients used higher standardized daily doses of opiates (68 mg vs 39 mg, median difference 24 mg, CI 7-42).
Conclusion: Proxies of hospitalized and non-hospitalized patients report high treatment satisfaction after opting for NOM. Non-hospitalization may have a beneficial effect on quality of dying in selected patients who have pre-recorded do-not-hospitalize directives or shared decision-making after a suspected hip fracture.
期刊介绍:
Acta Orthopaedica (previously Acta Orthopaedica Scandinavica) presents original articles of basic research interest, as well as clinical studies in the field of orthopedics and related sub disciplines. Ever since the journal was founded in 1930, by a group of Scandinavian orthopedic surgeons, the journal has been published for an international audience. Acta Orthopaedica is owned by the Nordic Orthopaedic Federation and is the official publication of this federation.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


