Population Pharmacokinetics of Cefepime in Critically Ill Children and Young Adults: Model Development and External Validation for Monte Carlo Simulations and Model-Informed Precision Dosing.
Ronaldo Morales Junior, H Rhodes Hambrick, Tomoyuki Mizuno, Kathryn E Pavia, Kelli M Paice, Peter Tang, Erin Schuler, Kelli A Krallman, Luana Johnson, Michaela Collins, Abigayle Gibson, Calise Curry, Jennifer Kaplan, Stuart Goldstein, Sonya Tang Girdwood
{"title":"Population Pharmacokinetics of Cefepime in Critically Ill Children and Young Adults: Model Development and External Validation for Monte Carlo Simulations and Model-Informed Precision Dosing.","authors":"Ronaldo Morales Junior, H Rhodes Hambrick, Tomoyuki Mizuno, Kathryn E Pavia, Kelli M Paice, Peter Tang, Erin Schuler, Kelli A Krallman, Luana Johnson, Michaela Collins, Abigayle Gibson, Calise Curry, Jennifer Kaplan, Stuart Goldstein, Sonya Tang Girdwood","doi":"10.1007/s40262-025-01485-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objective: </strong>This study aimed to develop a population pharmacokinetic model for cefepime in critically ill pediatric and young adult patients to inform dosing recommendations and to evaluate the model's predictive performance for model-informed precision dosing.</p><p><strong>Methods: </strong>Patients in the pediatric intensive care unit receiving cefepime were prospectively enrolled for clinical data collection and opportunistic plasma sampling for cefepime concentrations. Nonlinear mixed effects modeling was conducted using NONMEM. Allometric body weight scaling was included as a covariate with fixed exponents. Monte Carlo simulations determined optimal initial dosing regimens against susceptible pathogens. The model's predictions were evaluated with an external dataset.</p><p><strong>Results: </strong>Data from 510 samples across 100 patients were best fit with a two-compartment model with first-order elimination. Estimated glomerular filtration rate and cumulative percentage of fluid balance were identified as significant covariates on clearance and central volume of distribution, respectively. Internal validation showed no model misspecification. External validation confirmed that bias and precision for both population and individual predictions were within commonly accepted ranges. Monte Carlo simulations suggested that the usual dose of 50 mg/kg may require a 3-h infusion or a 6-h dosing interval to keep concentrations above the Pseudomonas aeruginosa minimum inhibitory concentration (≤ 8 mg/L) throughout the dosing interval for patients with normal or augmented renal clearance.</p><p><strong>Conclusion: </strong>A cefepime population pharmacokinetic model for critically ill pediatric patients was successfully developed, accounting for patient renal function, fluid status, and body size, using real-world data. The model was internally and externally validated for use in optimal dosing simulations and model-informed precision dosing.</p>","PeriodicalId":10405,"journal":{"name":"Clinical Pharmacokinetics","volume":" ","pages":"553-564"},"PeriodicalIF":4.0000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12041147/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pharmacokinetics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40262-025-01485-5","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/23 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and objective: This study aimed to develop a population pharmacokinetic model for cefepime in critically ill pediatric and young adult patients to inform dosing recommendations and to evaluate the model's predictive performance for model-informed precision dosing.
Methods: Patients in the pediatric intensive care unit receiving cefepime were prospectively enrolled for clinical data collection and opportunistic plasma sampling for cefepime concentrations. Nonlinear mixed effects modeling was conducted using NONMEM. Allometric body weight scaling was included as a covariate with fixed exponents. Monte Carlo simulations determined optimal initial dosing regimens against susceptible pathogens. The model's predictions were evaluated with an external dataset.
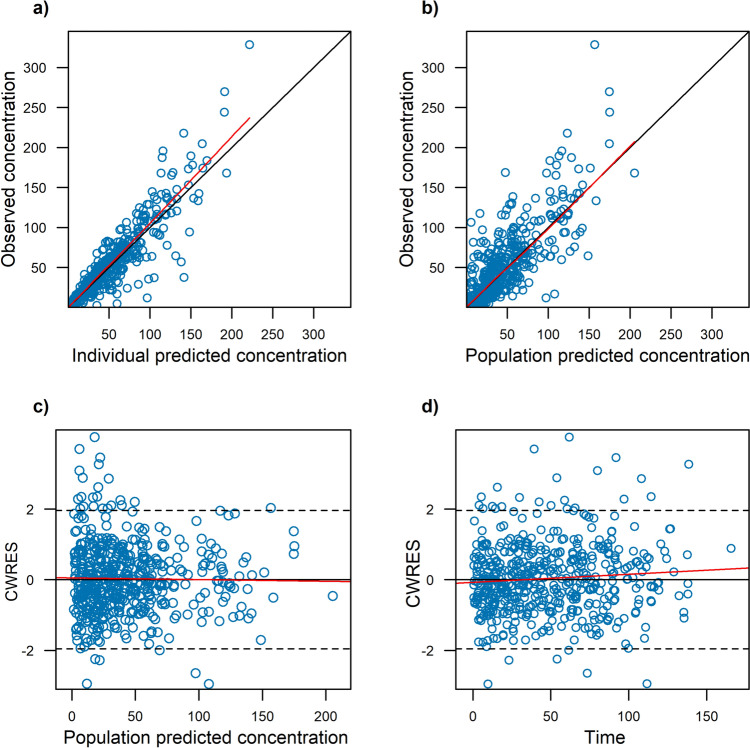
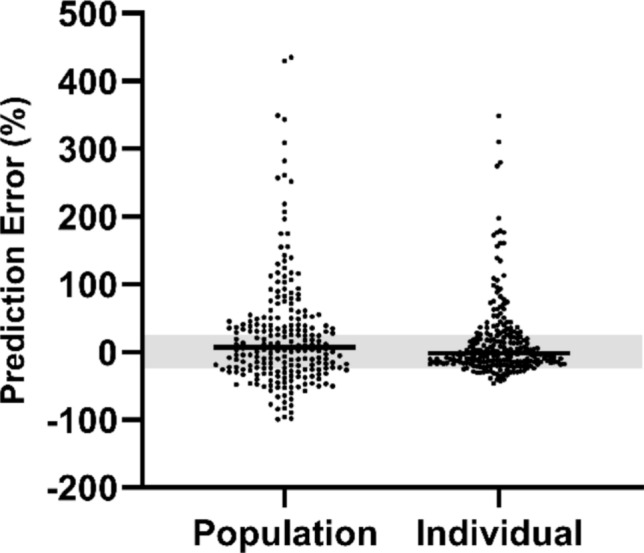
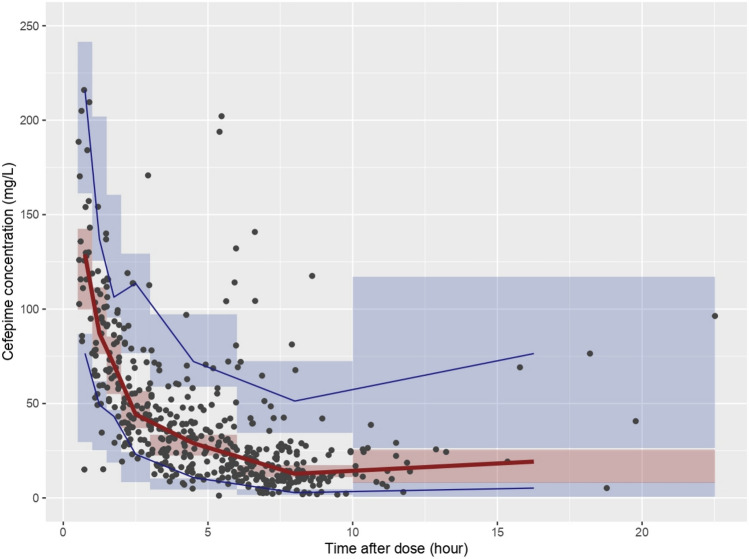
Results: Data from 510 samples across 100 patients were best fit with a two-compartment model with first-order elimination. Estimated glomerular filtration rate and cumulative percentage of fluid balance were identified as significant covariates on clearance and central volume of distribution, respectively. Internal validation showed no model misspecification. External validation confirmed that bias and precision for both population and individual predictions were within commonly accepted ranges. Monte Carlo simulations suggested that the usual dose of 50 mg/kg may require a 3-h infusion or a 6-h dosing interval to keep concentrations above the Pseudomonas aeruginosa minimum inhibitory concentration (≤ 8 mg/L) throughout the dosing interval for patients with normal or augmented renal clearance.
Conclusion: A cefepime population pharmacokinetic model for critically ill pediatric patients was successfully developed, accounting for patient renal function, fluid status, and body size, using real-world data. The model was internally and externally validated for use in optimal dosing simulations and model-informed precision dosing.
期刊介绍:
Clinical Pharmacokinetics promotes the continuing development of clinical pharmacokinetics and pharmacodynamics for the improvement of drug therapy, and for furthering postgraduate education in clinical pharmacology and therapeutics.
Pharmacokinetics, the study of drug disposition in the body, is an integral part of drug development and rational use. Knowledge and application of pharmacokinetic principles leads to accelerated drug development, cost effective drug use and a reduced frequency of adverse effects and drug interactions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


