Jack Lee, Maria Tomkins, Darran McDonald, Julie Martin-Grace, Claire Carthy, John Finnegan, Douglas Mulholland, Neal Dugal, Arnold D K Hill, Michael W O'Reilly, Mark Sherlock
{"title":"Resistant hypertension post-transsphenoidal surgery for pituitary Cushing's disease, leading to a diagnosis of primary aldosteronism.","authors":"Jack Lee, Maria Tomkins, Darran McDonald, Julie Martin-Grace, Claire Carthy, John Finnegan, Douglas Mulholland, Neal Dugal, Arnold D K Hill, Michael W O'Reilly, Mark Sherlock","doi":"10.1530/EDM-24-0137","DOIUrl":null,"url":null,"abstract":"<p><strong>Summary: </strong>We describe a case of a 42-year-old gentleman, 5 years post-transsphenoidal surgery (TSS) for pituitary-dependent Cushing's disease, initially presenting with malignant hypertension. Despite an initial improvement in his blood pressure post-TSS, he was found to be persistently hypertensive on follow-up despite no clinical or biochemical evidence of recurrence of hypercortisolism. His blood pressure remained elevated despite five antihypertensive agents. His renin concentration was <5 mIU/L (9-103.5) and aldosterone concentration was 877 pmol/L (0-670). A subsequent CT of the adrenals showed a 1.2 cm left adrenal nodule. He was not suitable for adrenal vein sampling (AVS) at this time due to difficult-to-control hypertension. Biochemistry was difficult to interpret in the context of a multitude of interfering medications, which were necessary given his difficult-to-control hypertension and hypokalaemia. Once suitable, his initial AVS was unsuccessful due to failure to cannulate the right adrenal vein. He was given the further options of repeat AVS vs 11C-metomidate PET vs medical management of his blood pressure. He proceeded with a repeat AVS, with successful cannulation of both adrenal veins. This showed evidence of hyperaldosteronism on the left side, with a lateralisation index of 39.5 and a contralateral suppression index of 0.28. He proceeded with a robotic left adrenalectomy, leading to significant improvement in his blood pressure, dropping from a mean reading of 142/85 during daytime and 150/88 mmHg at nighttime on five antihypertensive agents to normotensive levels of 114/77 mmHg on two agents.</p><p><strong>Learning points: </strong>It is important to consider a broad differential for uncontrolled hypertension. It must be considered that patients can present with multiple, isolated endocrinopathies. There are diagnostic challenges with primary aldosteronism, with medication regimens regularly effecting suitability of testing and interpretation of results. AVS can be a challenging procedure, leading to diagnostic challenges in the lateralisation of primary aldosteronism; however, it or another form of lateralisation is essential to guide management options.</p>","PeriodicalId":37467,"journal":{"name":"Endocrinology, Diabetes and Metabolism Case Reports","volume":"2025 1","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2025-02-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11883862/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrinology, Diabetes and Metabolism Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1530/EDM-24-0137","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"Print","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
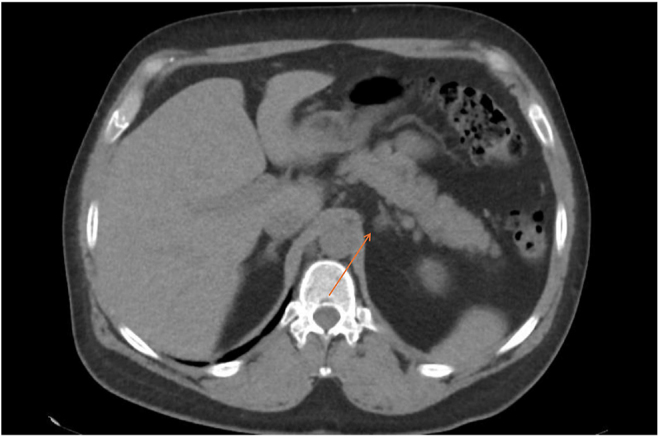
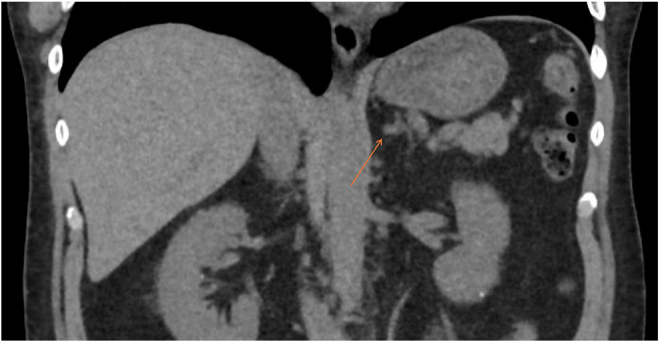
Summary: We describe a case of a 42-year-old gentleman, 5 years post-transsphenoidal surgery (TSS) for pituitary-dependent Cushing's disease, initially presenting with malignant hypertension. Despite an initial improvement in his blood pressure post-TSS, he was found to be persistently hypertensive on follow-up despite no clinical or biochemical evidence of recurrence of hypercortisolism. His blood pressure remained elevated despite five antihypertensive agents. His renin concentration was <5 mIU/L (9-103.5) and aldosterone concentration was 877 pmol/L (0-670). A subsequent CT of the adrenals showed a 1.2 cm left adrenal nodule. He was not suitable for adrenal vein sampling (AVS) at this time due to difficult-to-control hypertension. Biochemistry was difficult to interpret in the context of a multitude of interfering medications, which were necessary given his difficult-to-control hypertension and hypokalaemia. Once suitable, his initial AVS was unsuccessful due to failure to cannulate the right adrenal vein. He was given the further options of repeat AVS vs 11C-metomidate PET vs medical management of his blood pressure. He proceeded with a repeat AVS, with successful cannulation of both adrenal veins. This showed evidence of hyperaldosteronism on the left side, with a lateralisation index of 39.5 and a contralateral suppression index of 0.28. He proceeded with a robotic left adrenalectomy, leading to significant improvement in his blood pressure, dropping from a mean reading of 142/85 during daytime and 150/88 mmHg at nighttime on five antihypertensive agents to normotensive levels of 114/77 mmHg on two agents.
Learning points: It is important to consider a broad differential for uncontrolled hypertension. It must be considered that patients can present with multiple, isolated endocrinopathies. There are diagnostic challenges with primary aldosteronism, with medication regimens regularly effecting suitability of testing and interpretation of results. AVS can be a challenging procedure, leading to diagnostic challenges in the lateralisation of primary aldosteronism; however, it or another form of lateralisation is essential to guide management options.
期刊介绍:
Endocrinology, Diabetes & Metabolism Case Reports publishes case reports on common and rare conditions in all areas of clinical endocrinology, diabetes and metabolism. Articles should include clear learning points which readers can use to inform medical education or clinical practice. The types of cases of interest to Endocrinology, Diabetes & Metabolism Case Reports include: -Insight into disease pathogenesis or mechanism of therapy - Novel diagnostic procedure - Novel treatment - Unique/unexpected symptoms or presentations of a disease - New disease or syndrome: presentations/diagnosis/management - Unusual effects of medical treatment - Error in diagnosis/pitfalls and caveats


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


