Nicole Sunshine, Jenny Martinez, Alexandra Bazan, William R Wolowich, Tony Zitek
{"title":"Ketamine Versus Haloperidol/Lorazepam/Diphenhydramine Combination Treatment for Management of Acute Agitation in the Emergency Department.","authors":"Nicole Sunshine, Jenny Martinez, Alexandra Bazan, William R Wolowich, Tony Zitek","doi":"10.2147/OAEM.S486208","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Appropriate use and timing of agents for chemical management of patient agitation is critical for the safety of patients and providers. Ketamine may have a preferable safety profile in acutely agitated patients, especially those with an unknown medication history given that it does not carry the same cardiovascular and respiratory risks as other sedative agents currently used in practice. This study aimed to evaluate subsequent chemical sedation requirements and the incidence of adverse events following the use of ketamine for agitation as compared to combination antipsychotic/sedative use in the ED.</p><p><strong>Methods: </strong>This was a retrospective, single-center, observational cohort study of 102 adult patients who received chemical sedation for agitation/aggression/combative behavior from January 2018 to December 2023 at the Mount Sinai Medical Center Emergency Department. Patients who received at least one dose of ketamine (n = 51) were compared to patients who received at least one dose of the B52 combination (diphenhydramine (Benadryl) 25 mg, haloperidol (Haldol) 5 mg, and lorazepam (Ativan) 2 mg) (n = 51) for management of aggression. The primary endpoint was restricted mean survival time (RMST) to next sedative given. Secondary endpoints included the number of additional sedatives needed, adverse events, and length of stay.</p><p><strong>Results: </strong>The use of ketamine was associated with patients requiring additional sedation both more often and sooner than patients who received the B52 combination (RMST to next sedative: 2.1 hours ketamine vs 4 hours B52; <i>p</i> = 0.032, median additional doses: 3 doses ketamine group vs 0 doses B52 group; <i>p</i> < 0.00).</p><p><strong>Conclusion: </strong>In agitated patients within the ED, the administration of ketamine demonstrated inadequate duration of sedation and increased need for supplemental sedative use compared to B52.</p>","PeriodicalId":45096,"journal":{"name":"Open Access Emergency Medicine","volume":"17 ","pages":"113-120"},"PeriodicalIF":1.5000,"publicationDate":"2025-02-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11840334/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Access Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/OAEM.S486208","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Appropriate use and timing of agents for chemical management of patient agitation is critical for the safety of patients and providers. Ketamine may have a preferable safety profile in acutely agitated patients, especially those with an unknown medication history given that it does not carry the same cardiovascular and respiratory risks as other sedative agents currently used in practice. This study aimed to evaluate subsequent chemical sedation requirements and the incidence of adverse events following the use of ketamine for agitation as compared to combination antipsychotic/sedative use in the ED.
Methods: This was a retrospective, single-center, observational cohort study of 102 adult patients who received chemical sedation for agitation/aggression/combative behavior from January 2018 to December 2023 at the Mount Sinai Medical Center Emergency Department. Patients who received at least one dose of ketamine (n = 51) were compared to patients who received at least one dose of the B52 combination (diphenhydramine (Benadryl) 25 mg, haloperidol (Haldol) 5 mg, and lorazepam (Ativan) 2 mg) (n = 51) for management of aggression. The primary endpoint was restricted mean survival time (RMST) to next sedative given. Secondary endpoints included the number of additional sedatives needed, adverse events, and length of stay.
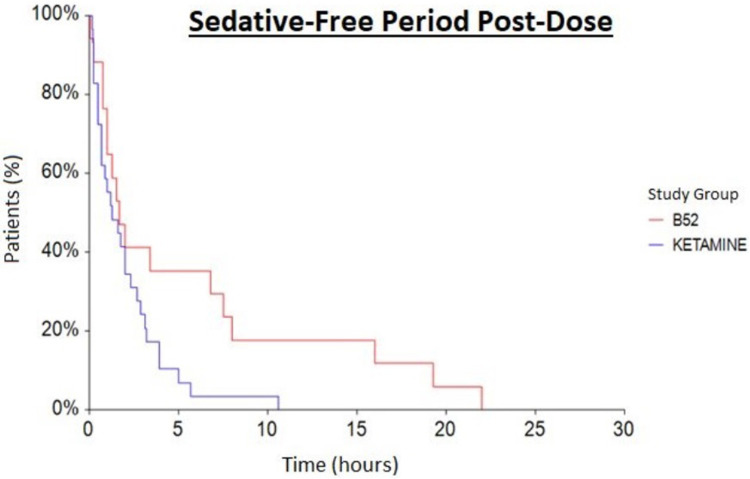
Results: The use of ketamine was associated with patients requiring additional sedation both more often and sooner than patients who received the B52 combination (RMST to next sedative: 2.1 hours ketamine vs 4 hours B52; p = 0.032, median additional doses: 3 doses ketamine group vs 0 doses B52 group; p < 0.00).
Conclusion: In agitated patients within the ED, the administration of ketamine demonstrated inadequate duration of sedation and increased need for supplemental sedative use compared to B52.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


