Andreas Angelopoulos, Ioannis Kouverianos, Dimitrios Daoussis
{"title":"The Paradox of Osteoporosis in Spondyloarthropathies.","authors":"Andreas Angelopoulos, Ioannis Kouverianos, Dimitrios Daoussis","doi":"10.31138/mjr.270924.poa","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Spondyloarthropathies (SpA) are a family of inflammatory disorders that affect the spine and peripheral joints. The most common representatives are axial Spondylarthritis (axSpA) and Psoriatic Arthritis (PsA). Despite the fact that SpA are characterised by new bone formation, paradoxically, total Bone Mineral Density (BMD) may be decreased.</p><p><strong>Methods: </strong>An electronic search was conducted on Medline in order to explore the prevalence, risk factors and pathophysiology of Osteoporosis (OP) in SpA patients.</p><p><strong>Results: </strong>The prevalence of OP globally is reported to be 18.3%. The prevalence of OP in Axial Spondylarthritis (axSpA) patients ranges from 11.7% to 34.4%, while in Psoriatic Arthritis (PsA) patients seems to be similar to the general population. Several factors have been proposed for the development of OP in SpA, such as corticosteroid use and physical inactivity. Moreover, systemic inflammation appears to participate in the pathophysiology of OP with inflammatory cytokines such as Tumour Necrosis Factor (TNF) and Interleukin (IL)-23/IL-17 potentially having a key role in the pathogenesis of bone loss.</p><p><strong>Discussion: </strong>The current literature points to the direction that OP is an established comorbidity in axSpA. Local or/and systemic inflammation is possibly the main pathway contributing to bone loss in axSpA patients. However, it remains unclear whether OP is an established comorbidity in PsA patients, as it seems that OP is a treatment-associated adverse event.</p>","PeriodicalId":32816,"journal":{"name":"Mediterranean Journal of Rheumatology","volume":"35 Suppl 3","pages":"528-533"},"PeriodicalIF":0.0000,"publicationDate":"2024-12-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11834996/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Mediterranean Journal of Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31138/mjr.270924.poa","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
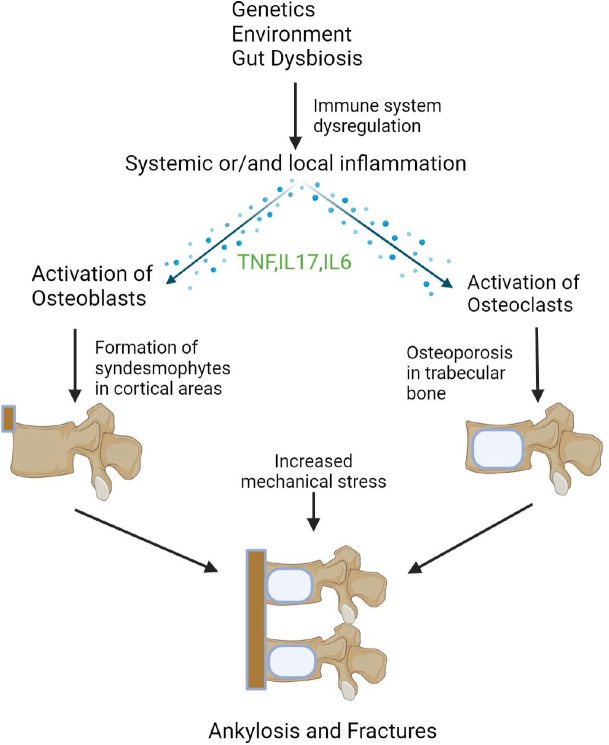
Introduction: Spondyloarthropathies (SpA) are a family of inflammatory disorders that affect the spine and peripheral joints. The most common representatives are axial Spondylarthritis (axSpA) and Psoriatic Arthritis (PsA). Despite the fact that SpA are characterised by new bone formation, paradoxically, total Bone Mineral Density (BMD) may be decreased.
Methods: An electronic search was conducted on Medline in order to explore the prevalence, risk factors and pathophysiology of Osteoporosis (OP) in SpA patients.
Results: The prevalence of OP globally is reported to be 18.3%. The prevalence of OP in Axial Spondylarthritis (axSpA) patients ranges from 11.7% to 34.4%, while in Psoriatic Arthritis (PsA) patients seems to be similar to the general population. Several factors have been proposed for the development of OP in SpA, such as corticosteroid use and physical inactivity. Moreover, systemic inflammation appears to participate in the pathophysiology of OP with inflammatory cytokines such as Tumour Necrosis Factor (TNF) and Interleukin (IL)-23/IL-17 potentially having a key role in the pathogenesis of bone loss.
Discussion: The current literature points to the direction that OP is an established comorbidity in axSpA. Local or/and systemic inflammation is possibly the main pathway contributing to bone loss in axSpA patients. However, it remains unclear whether OP is an established comorbidity in PsA patients, as it seems that OP is a treatment-associated adverse event.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


