Sarah Alsadiq, Adi Kartolo, Elaine McWhirter, Wilma Hopman, Tara Baetz
{"title":"Efficacy and safety of adjuvant systemic therapies in trial non-eligible resected stages III and IV melanoma patients.","authors":"Sarah Alsadiq, Adi Kartolo, Elaine McWhirter, Wilma Hopman, Tara Baetz","doi":"10.1080/20450885.2025.2461963","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Adjuvant immunotherapy and targeted therapy are now the standard of care for patients with resected stage IIIA-IV melanoma. However, little is known regarding its efficacy in real-world patients who were not represented in these landmark trials.</p><p><strong>Methods: </strong>This retrospective study included all patients with resected stage IIIA-IV melanoma who received adjuvant systemic therapy between January 1 2018 and December 31 2020, in two Canadian academic cancer. Primary outcome was the proportion of trial non-eligible patients in the real-world setting. Survival and safety analyses were also conducted.</p><p><strong>Results: </strong>Of the total 113 patient, 99 (88%) were trial non-eligible patients. Most common reasons for trial non-eligible criteria was having no baseline CLND (72%), followed by outside of treatment window >12 weeks (30%), stage IIIA (14%), unknown primary (9%), stage IV (14%), and baseline AD on immunosuppressants (3%). There were no significant RFS (P = 0.731) or OS (P = 0.110) differences in the overall population of trial eligible vs. non-eligible. Safety profiles were similar between the trial eligible vs. non-eligible groups.</p><p><strong>Conclusion: </strong>Our study suggested a high proportion of real-world patients would have been deemed non-eligible for clinical trials. Regardless, adjuvant systemic therapy delivered similar survival and toxicity outcomes in both groups.</p>","PeriodicalId":44562,"journal":{"name":"Melanoma Management","volume":"12 1","pages":"2461963"},"PeriodicalIF":0.7000,"publicationDate":"2025-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11834428/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Melanoma Management","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/20450885.2025.2461963","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/17 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Adjuvant immunotherapy and targeted therapy are now the standard of care for patients with resected stage IIIA-IV melanoma. However, little is known regarding its efficacy in real-world patients who were not represented in these landmark trials.
Methods: This retrospective study included all patients with resected stage IIIA-IV melanoma who received adjuvant systemic therapy between January 1 2018 and December 31 2020, in two Canadian academic cancer. Primary outcome was the proportion of trial non-eligible patients in the real-world setting. Survival and safety analyses were also conducted.
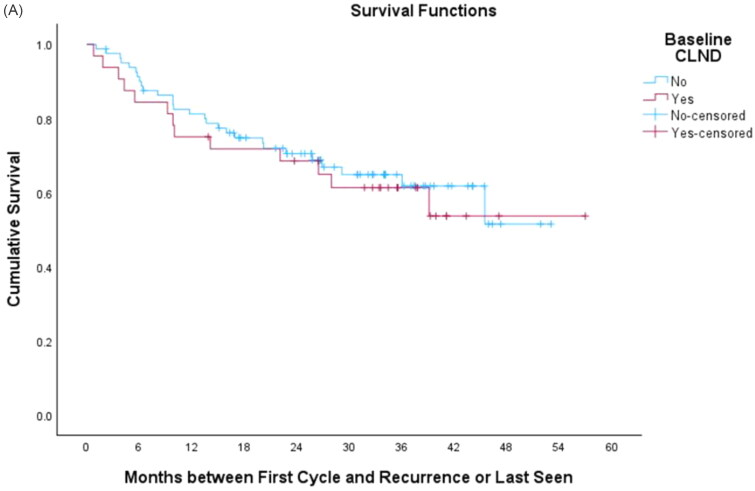
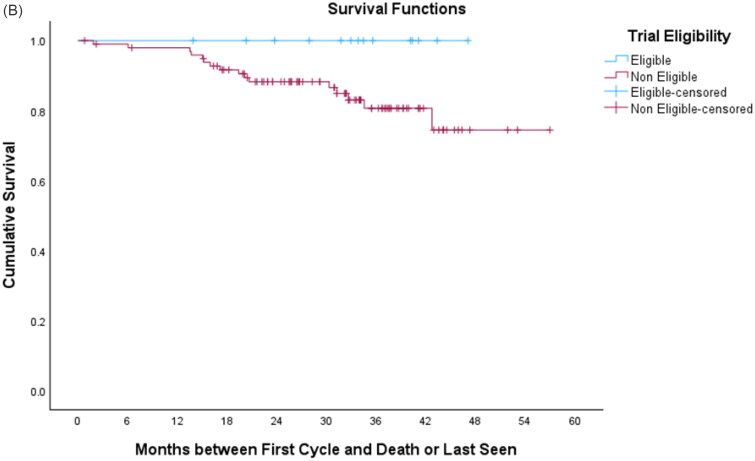
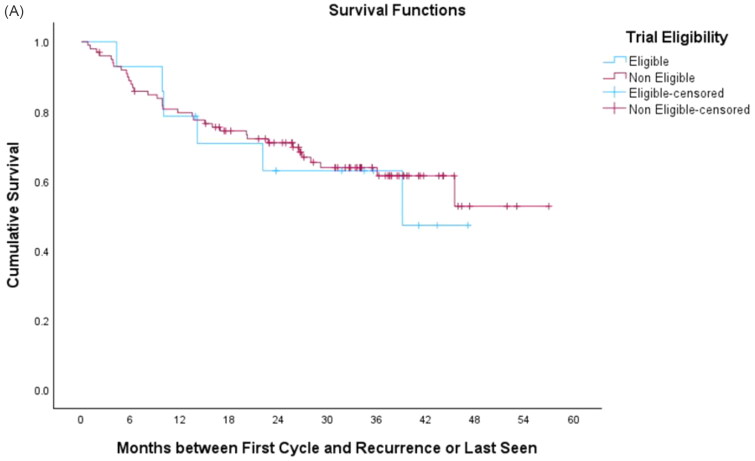
Results: Of the total 113 patient, 99 (88%) were trial non-eligible patients. Most common reasons for trial non-eligible criteria was having no baseline CLND (72%), followed by outside of treatment window >12 weeks (30%), stage IIIA (14%), unknown primary (9%), stage IV (14%), and baseline AD on immunosuppressants (3%). There were no significant RFS (P = 0.731) or OS (P = 0.110) differences in the overall population of trial eligible vs. non-eligible. Safety profiles were similar between the trial eligible vs. non-eligible groups.
Conclusion: Our study suggested a high proportion of real-world patients would have been deemed non-eligible for clinical trials. Regardless, adjuvant systemic therapy delivered similar survival and toxicity outcomes in both groups.
期刊介绍:
Skin cancer is on the rise. According to the World Health Organization, 132,000 melanoma skin cancers occur globally each year. While early-stage melanoma is usually relatively easy to treat, once disease spreads prognosis worsens considerably. Therefore, research into combating advanced-stage melanoma is a high priority. New and emerging therapies, such as monoclonal antibodies, B-RAF and KIT inhibitors, antiangiogenic agents and novel chemotherapy approaches hold promise for prolonging survival, but the search for a cure is ongoing. Melanoma Management publishes high-quality peer-reviewed articles on all aspects of melanoma, from prevention to diagnosis and from treatment of early-stage disease to late-stage melanoma and metastasis. The journal presents the latest research findings in melanoma research and treatment, together with authoritative reviews, cutting-edge editorials and perspectives that highlight hot topics and controversy in the field. Independent drug evaluations assess newly approved medications and their role in clinical practice. Key topics covered include: Risk factors, prevention and sun safety education Diagnosis, staging and grading Surgical excision of melanoma lesions Sentinel lymph node biopsy Biological therapies, including immunotherapy and vaccination Novel chemotherapy options Treatment of metastasis Prevention of recurrence Patient care and quality of life.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


