{"title":"Clinical and ethical perspectives of ovarian stimulation and oocyte cryopreservation in adolescents: 6 years experience from a tertiary centre.","authors":"Sania Latif, Melanie Davies, Emily Vaughan, Dimitrios Mavrelos, Stuart Lavery, Ephia Yasmin","doi":"10.1093/hropen/hoaf005","DOIUrl":null,"url":null,"abstract":"<p><strong>Study question: </strong>What are the clinical and ethical challenges of performing ovarian stimulation and oocyte cryopreservation in adolescents and the barriers to providing treatment?</p><p><strong>Summary answer: </strong>Our study shows that, in one of the largest case series to date in this population, post-pubertal adolescents as young as age 13 years can undergo ovarian stimulation and oocyte cryopreservation with a response comparable to adults.</p><p><strong>What is known already: </strong>Fertility preservation in adolescents has not been well studied, with little data available in the existing literature. Referrals for fertility preservation in adolescents are increasing due to developments in childhood cancer treatments, which have led to a growing population of children at risk of developing premature ovarian insufficiency. Those with certain benign conditions or gender incongruence also face this challenge. All established fertility preservation guidelines state that where there is a risk to fertility, oocyte cryopreservation should be offered to post-pubertal females. However, counselling and consenting young people about fertility decisions is an ethically complex area, and assessing capacity to consent in this age group is not straightforward.</p><p><strong>Study design size duration: </strong>This was a retrospective observational cohort study of 182 referrals for fertility preservation counselling to a specialist unit, and we present outcomes for the 33 adolescents who underwent 36 cycles of ovarian stimulation and oocyte cryopreservation between January 2018 and January 2024.</p><p><strong>Participants/materials setting methods: </strong>We included patients aged 13-18 years who underwent ovarian stimulation and oocyte cryopreservation for fertility preservation due to high or intermediate risk of gonadotoxicity from medical or surgical treatment at a public-funded specialist unit. The primary outcome was oocyte yield; secondary outcomes included oocyte maturity rate, complications, and dropout rate. Data were retrieved from a prospectively managed database.</p><p><strong>Main results and the role of chance: </strong>There was a total of 182 referrals received, and of these, 33 patients underwent 36 cycles of ovarian stimulation and oocyte cryopreservation. Indications for fertility preservation included malignancy <i>n</i> = 19/36 (54%), ovarian cyst surgery <i>n</i> = 7/36 (19%), immunological disorders <i>n</i> = 4/36 (11%), benign haematological disease <i>n</i> = 2/36 (6%), gender reassignment treatment <i>n</i> = 3/36 (8%), and genetic conditions <i>n</i> = 1/36 (3%). The youngest child who underwent ovarian stimulation was aged 13 years and 10 months at the time of egg collection; the minimum time from menarche to ovarian stimulation was 4 months, the median AMH (anti-Müllerian hormone) was 16.7 pmol/l (range 2.8-36.9 pmol/l), and the antral follicle count (AFC) was 11 (3-36). The median number of cryopreserved oocytes was 14 (range 4-39), and the oocyte maturity rate was 85% (35-100%). Ultrasound monitoring was performed transabdominally in 5/33 (15%) and transvaginally in 28/33 (85%). Egg collection was performed transvaginally in all cases in this cohort. All cycles proceeded to completion. All adolescents were counselled in association with a family member to obtain informed consent, and all were assessed as able to comprehend discussions.</p><p><strong>Limitations reasons for caution: </strong>In view of concerns regarding increased aneuploidy rates in this age group compared to women in their twenties, there is a need for long-term outcome studies expanding on our findings with data on livebirths to support clinicians needing to counsel patients and perform oocyte cryopreservation in adolescents.</p><p><strong>Wider implications of the findings: </strong>Clinician experience, correct setting, and availability of funding will enable a permissive environment for oocyte cryopreservation in adolescents. In our experience, transvaginal egg collection is an accepted procedure when counselled appropriately.</p><p><strong>Study funding/competing interests: </strong>No funding was received for this work. No competing interests are declared.</p><p><strong>Trial registration number: </strong>N/A.</p>","PeriodicalId":73264,"journal":{"name":"Human reproduction open","volume":"2025 1","pages":"hoaf005"},"PeriodicalIF":11.1000,"publicationDate":"2025-01-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11825388/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Human reproduction open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/hropen/hoaf005","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Study question: What are the clinical and ethical challenges of performing ovarian stimulation and oocyte cryopreservation in adolescents and the barriers to providing treatment?
Summary answer: Our study shows that, in one of the largest case series to date in this population, post-pubertal adolescents as young as age 13 years can undergo ovarian stimulation and oocyte cryopreservation with a response comparable to adults.
What is known already: Fertility preservation in adolescents has not been well studied, with little data available in the existing literature. Referrals for fertility preservation in adolescents are increasing due to developments in childhood cancer treatments, which have led to a growing population of children at risk of developing premature ovarian insufficiency. Those with certain benign conditions or gender incongruence also face this challenge. All established fertility preservation guidelines state that where there is a risk to fertility, oocyte cryopreservation should be offered to post-pubertal females. However, counselling and consenting young people about fertility decisions is an ethically complex area, and assessing capacity to consent in this age group is not straightforward.
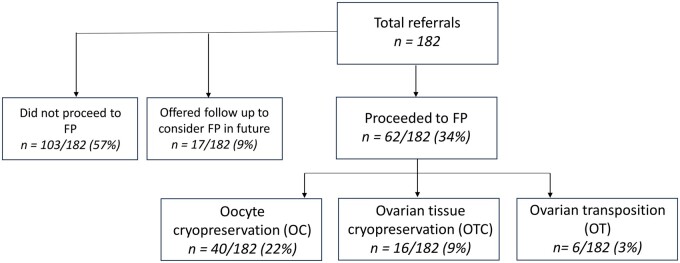
Study design size duration: This was a retrospective observational cohort study of 182 referrals for fertility preservation counselling to a specialist unit, and we present outcomes for the 33 adolescents who underwent 36 cycles of ovarian stimulation and oocyte cryopreservation between January 2018 and January 2024.
Participants/materials setting methods: We included patients aged 13-18 years who underwent ovarian stimulation and oocyte cryopreservation for fertility preservation due to high or intermediate risk of gonadotoxicity from medical or surgical treatment at a public-funded specialist unit. The primary outcome was oocyte yield; secondary outcomes included oocyte maturity rate, complications, and dropout rate. Data were retrieved from a prospectively managed database.
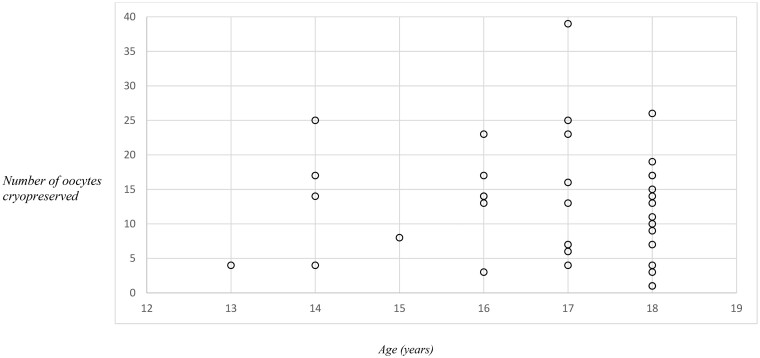
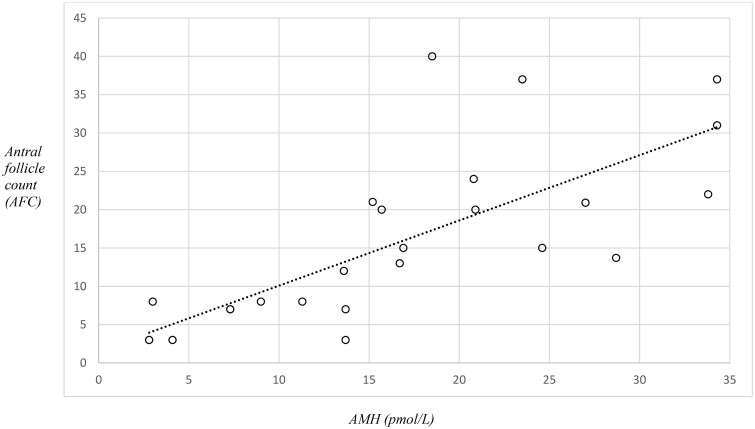
Main results and the role of chance: There was a total of 182 referrals received, and of these, 33 patients underwent 36 cycles of ovarian stimulation and oocyte cryopreservation. Indications for fertility preservation included malignancy n = 19/36 (54%), ovarian cyst surgery n = 7/36 (19%), immunological disorders n = 4/36 (11%), benign haematological disease n = 2/36 (6%), gender reassignment treatment n = 3/36 (8%), and genetic conditions n = 1/36 (3%). The youngest child who underwent ovarian stimulation was aged 13 years and 10 months at the time of egg collection; the minimum time from menarche to ovarian stimulation was 4 months, the median AMH (anti-Müllerian hormone) was 16.7 pmol/l (range 2.8-36.9 pmol/l), and the antral follicle count (AFC) was 11 (3-36). The median number of cryopreserved oocytes was 14 (range 4-39), and the oocyte maturity rate was 85% (35-100%). Ultrasound monitoring was performed transabdominally in 5/33 (15%) and transvaginally in 28/33 (85%). Egg collection was performed transvaginally in all cases in this cohort. All cycles proceeded to completion. All adolescents were counselled in association with a family member to obtain informed consent, and all were assessed as able to comprehend discussions.
Limitations reasons for caution: In view of concerns regarding increased aneuploidy rates in this age group compared to women in their twenties, there is a need for long-term outcome studies expanding on our findings with data on livebirths to support clinicians needing to counsel patients and perform oocyte cryopreservation in adolescents.
Wider implications of the findings: Clinician experience, correct setting, and availability of funding will enable a permissive environment for oocyte cryopreservation in adolescents. In our experience, transvaginal egg collection is an accepted procedure when counselled appropriately.
Study funding/competing interests: No funding was received for this work. No competing interests are declared.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


